REVIEW
www.advancedscience.com
Toward the Clinical Translation of Implantable
Brain–Computer Interfaces for Motor Impairment: Research
Trends and Outcome Measures
Esmee Dohle, Eleanor Swanson, Luka Jovanovic, Suraya Yusuf, Lucy Thompson,
Hugo Layard Horsfall, William Muirhead, Luke Bashford, and Jamie Brannigan*
1. Introduction
Implantable brain–computer interfaces (iBCIs) decode neural signals to
control external effectors, offering potential to restore function in individuals Millions of individuals worldwide suffer
from neurological conditions which im-
with severe motor impairments, such as loss of limb function or speech. This
pair the transmission of motor intentions
systematic review examines the evolution of iBCI research and key from the brain to muscles, preventing them
bottlenecks to clinical translation, particularly the absence of standardized, from independently performing activities of
clinically meaningful outcome measures. A comprehensive search of daily living (ADL). The disease burden of
MEDLINE, Embase, and CINAHL identifies 112 studies, nearly half (49.1%) such conditions, which include stroke, amy-
otrophic lateral sclerosis (ALS), and spinal
published since 2020. Eighty unique iBCI participants were identified,
cord injury (SCI), is rapidly increasing,
providing the most up-to-date estimate of global users. Research remains with neurological diseases now the lead-
concentrated in the United States (83%), with growing contributions from ing cause of ill health worldwide.[1] Further-
Europe, China, and Australia. Electrocorticography (ECoG)-based devices more, most individuals with SCI sustain
increasingly emerge alongside micro-electrode arrays. iBCI devices are now their injury before the age of 50, resulting in
being used to control a broader range of effectors, including robotic decades with increased dependence on care
and reduced quality of life.[2–4]
prosthetics and digital technologies. Although most (69.6%) studies reported
In recent decades, brain–computer inter-
outcome measures prospectively, these primarily related to decoding (69.6%) faces (BCIs) have emerged as a transforma-
and task performance (62.5%), with only 17.9% assessing clinical outcomes. tive technology to restore function by de-
When cassessed, clinical outcomes were highly heterogeneous due to varied coding preserved neural signals and trans-
approaches across target populations. iBCIs show potential to restore mitting this activity via computers to effec-
tor devices, enabling the performance of
functional independence at scale. However, challenges remain
desired actions. These prosthetic systems
around cross-subject generalization, scalable implantation, and outcome function by recording neural signals, de-
standardization. Novel measures should be developed collaboratively with coding the signals into desired output ac-
engineers, clinicians, and individuals with lived experience of motor tions, and executing these actions via an ef-
impairment. fector in the environment. Various systems
have been investigated to accomplish each
E. Dohle, S. Yusuf, J. Brannigan L. Jovanovic
Oxford University Hospitals East and North Hertfordshire NHS Trust
John Radcliffe Hospital Lister Hospital
Oxford OX3 9DU, UK Stevenage SG1 4AB, UK
E-mail: L. Thompson
E. Swanson Faculty of Medicine
Utrecht University Medical Centre Imperial College London
Utrecht 3584 CX, Netherlands London SW7 5NH, UK
H. L. Horsfall, W. Muirhead
Department of Neurosurgery
National Hospital for Neurology and Neurosurgery
The ORCID identification number(s) for the author(s) of this article London WC1N 3BG, UK
can be found under https://doi.org/10.1002/advs.202501912 H. L. Horsfall, W. Muirhead
The Francis Crick Institute
© 2025 The Author(s). Advanced Science published by Wiley-VCH
London NW1 1AT, UK
GmbH. This is an open access article under the terms of the Creative
Commons Attribution License, which permits use, distribution and H. L. Horsfall, W. Muirhead
reproduction in any medium, provided the original work is properly cited. Institute of Neurology
University College London
DOI: 10.1002/advs.202501912 London WC1N 3BG, UK
Adv. Sci. 2025, 12, e01912 e01912 (1 of 19) © 2025 The Author(s). Advanced Science published by Wiley-VCH GmbH
, 21983844, 2025, 32, Downloaded from https://advanced.onlinelibrary.wiley.com/doi/10.1002/advs.202501912 by Francis Crick Institute, Wiley Online Library on [04/09/2025]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
www.advancedsciencenews.com www.advancedscience.com
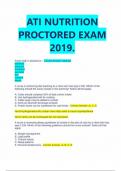
Figure 1. Example of experimental setup of an implantable brain–computer interface with a digital effector.
of these steps. Sensors may be implanted intracranially, such as sory feedback.[18,20–22] Although non-implantable BCI paradigms
micro-electrode arrays (MEAs), surface ECoG arrays, or endovas- using EEG have demonstrated clinical benefit,[23] and impor-
cular stent arrays. Alternatively, sensing may be non-implantable, tant progress has been made in enabling digital control,[24,25] ex-
using wearable device techniques like scalp electroencephalogra- tracranial electrical recording is limited by several factors. These
phy (EEG) and functional near-infrared spectroscopy (fNIRS).[5] include poor spatial discrimination, low-pass filtering in the
Decoding of neural signals may be performed using a vari- frequency domain resulting from the transmission of signals
ety of neural signal processing techniques. Outputs can drive through the skull, and the requirement for skin abrasion during
a range of effectors, including robotic prosthetic limbs,[6–8] vir- routine setup of extracranial sensors to enable clinically useable
tual avatars,[9–11] consumer digital devices,[12–15] and decoded recordings.
speech.[16–19] A typical BCI system with a digital device effector is Building on advances in implantable BCIs, there are numer-
shown in Figure 1. This is an example of an implantable system ous academic and commercial efforts to translate these systems
requiring a percutaneous connection, which has been commonly at scale and restore functional independence for individuals with
used in research settings to make seminal engineering and sci- motor impairments as part of routine clinical practice.[15,26] How-
entific advances in recent decades.[19,20] ever, no iBCI technology has yet received regulatory approval for
Implantable BCI (iBCI) systems have yielded significant clini- clinical use or been integrated into standard clinical practice. A
cal and engineering breakthroughs. This includes the first long- major challenge in the clinical translation of iBCI devices is the
term independent device use at home (in a controlled, clinical absence of consensus for clinically meaningful outcome mea-
trial setting), computer cursor control, high-dimensional pros- sures that can be used when evaluating device efficacy in clinical
thetic limb control, restoration of own muscle control via func- trials.[27,28] In the USA, the Food and Drug Administration has
tional electrical stimulation or spinal cord stimulation, high- highlighted the absence of an appropriate outcome measure[29]
speed communication output rates, and delivery of somatosen- and government funding has been awarded to investigate this.[30]
In this review, we present the largest and most up-to-date es-
timate of iBCI clinical trial participants worldwide, drawing on
data from 112 studies and integrating both published and veri-
L. Bashford fied unpublished sources. Unlike previous reviews that include
Bioscience Institute, Faculty of Medical Sciences
Newcastle University early-stage applications in contexts such as epilepsy,[31] the scope
Newcastle upon Tyne NE1 7RU, UK of our analysis is deliberately confined to clinical trials involv-
L. Bashford ing target populations with motor impairments, which includes
Department of Neurosurgery loss of limb function and/or speech. By focusing on individu-
University of Colorado als with ALS, SCI, and stroke, this review directly addresses the
Denver, CO 80045, USA
cohorts that stand to benefit most from the clinical translation
J. Brannigan
Department of Medical Physics and Biomedical Engineering
of iBCI technology. We establish a comprehensive registry not
University College London only as a new benchmark for assessing the global status of iBCI
London WC1E 6BT, UK trials, but also to serve as an essential resource for stakehold-
Adv. Sci. 2025, 12, e01912 e01912 (2 of 19) © 2025 The Author(s). Advanced Science published by Wiley-VCH GmbH
, 21983844, 2025, 32, Downloaded from https://advanced.onlinelibrary.wiley.com/doi/10.1002/advs.202501912 by Francis Crick Institute, Wiley Online Library on [04/09/2025]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
www.advancedsciencenews.com www.advancedscience.com
ers aiming to advance these technologies toward routine clinical Table 1. Exclusion criteria.
use.
To contextualize the field, we first map the evolution of iBCI Exclusion criteria
research trends, chronicling both the technical advances over 1 No use of implantable BCI devices
time and the heterogeneity in approaches that have contributed 2 Not a full text, independent publication
to the current challenges. We critically examine a key factor lim-
3 Not a primary study
iting clinical translation, namely the heterogeneity of outcome
4 Text not available in English
measures currently used to assess iBCI performance. We pro-
5 Full text not available
pose forward-looking solutions to the selection of appropriate
and standardized outcome measures, intending to extend the dis- 6 Non-human subjects
cussion to a multidisciplinary audience and accelerate the inte-
gration of iBCIs into standard clinical practice.
Cochlear implants were sensory prostheses which neither record
neural activity nor control external devices, and hence were not
included in this study.[36,37] Studies conducted in which there was
2. Experimental Section transient device implantation with a primary aim to aid peri-
This review was conducted in accordance with the pre- operative planning, for example, for seizure localization, were
ferred reporting items for systematic reviews and meta-analysis considered beyond the scope of this review. All full-text primary
(PRISMA) 2020 guidelines.[32] A completed checklist is included research papers in English were considered. Studies reporting
in the Materials SA (Supporting Information). This systematic exclusively on non-human subjects were excluded. An overview
review was prospectively registered on Open Science Framework of the exclusion hierarchy as provided to reviewers is shown in
(OSF) (https://osf.io/deyrj). Table 1.
2.4. Data Management, Extraction, and Appraisal
2.1. Search Strategy
Records were deduplicated using Rayyan.[38] Subsequently,
A sensitive search strategy was developed which combined syn-
records were blinded and screened by title and abstract by two in-
onyms for BCIs, intracortical, and patient, in consultation with
dependent reviewers. Full-text screening and data extraction were
a senior medical librarian. The search was applied to MEDLINE,
performed using a piloted data extraction proforma in MS Excel.
Embase and CINAHL using Ovid (Wolters Kluwer, Netherlands),
Risk of bias was assessed by two reviewers using the Mixed Meth-
and run from inception to 24th December 2024. The search strat-
ods Appraisal Tool checklist. Reference management was done
egy is included in Materials SB (Supporting Information). Fur-
using Zotero.
ther studies were identified through searching reference lists of
included records and searching the Google Scholar profiles of key
principal investigators in the field. 2.5. Data Synthesis
Analysis was performed in R (R Core Team, 2019) using the Tidy-
2.2. Study Selection verse package. As many participants were reported on in multiple
studies, the included studies were cross-referenced to match the
Included records were screened by two independent reviewers same participants across studies and prevent duplication of de-
(ED, ES). An initial pilot screen of 50 records was carried out to mographic details.[39] Plots were produced in R using the ggplot2
ensure concordance, following which reviewers were blinded to package.[40] Open-source R code shared in a previous publication
each other’s decisions using Rayyan (Rayyan Systems Inc, Cam- was adapted to create the map seen in Figure 2.[41] Graphics were
bridge, MA, USA). Disagreements were resolved by consensus produced using Inkscape (Inkscape Project, 2020).
or discussion with a third reviewer (JB). Full-text screening was Publications were grouped in 5-year intervals. Figures 3 and 4
carried out by the same reviewers (ED, ES). and 7, which show the proportions of different categories over
time, excluded time intervals with ≤3 published studies.
A subgroup analysis was carried out on studies which reported
2.3. Inclusion and Exclusion Criteria the use of iBCIs for communication purposes, either via cursor-
controlled typing or speech phoneme decoding paradigms. To
Studies were considered if they demonstrated the use of im- compare changes in achieved communication speed across stud-
plantable BCI devices with an intracranial sensing component ies over time, correct characters per minute (CCPM) estimates
and effector. For the purpose of this review, an implantable BCI were converted to words per minute (WPM) using the commonly
was defined as an intracranial device which records neural activ- used conversion factor of WPM = CPM/5. When speed was re-
ity representing volitional motor intent, such as intended limb ported in terms of characters per minute, it was combined with
movement or speech, and decoded this into an output signal to the reported error rate to calculate an estimate of correct charac-
control an external effector.[25] Non-implantable BCIs were pre- ters per minute. For each participant, the highest achieved mean
viously discussed in detail and had a limited potential to pro- speed was used, even if aided by additional technology, for exam-
vide clinically meaningful restoration of motor function.[5,33–35] ple, predictive typing or altered keyboard layouts. Accuracy was
Adv. Sci. 2025, 12, e01912 e01912 (3 of 19) © 2025 The Author(s). Advanced Science published by Wiley-VCH GmbH
www.advancedscience.com
Toward the Clinical Translation of Implantable
Brain–Computer Interfaces for Motor Impairment: Research
Trends and Outcome Measures
Esmee Dohle, Eleanor Swanson, Luka Jovanovic, Suraya Yusuf, Lucy Thompson,
Hugo Layard Horsfall, William Muirhead, Luke Bashford, and Jamie Brannigan*
1. Introduction
Implantable brain–computer interfaces (iBCIs) decode neural signals to
control external effectors, offering potential to restore function in individuals Millions of individuals worldwide suffer
from neurological conditions which im-
with severe motor impairments, such as loss of limb function or speech. This
pair the transmission of motor intentions
systematic review examines the evolution of iBCI research and key from the brain to muscles, preventing them
bottlenecks to clinical translation, particularly the absence of standardized, from independently performing activities of
clinically meaningful outcome measures. A comprehensive search of daily living (ADL). The disease burden of
MEDLINE, Embase, and CINAHL identifies 112 studies, nearly half (49.1%) such conditions, which include stroke, amy-
otrophic lateral sclerosis (ALS), and spinal
published since 2020. Eighty unique iBCI participants were identified,
cord injury (SCI), is rapidly increasing,
providing the most up-to-date estimate of global users. Research remains with neurological diseases now the lead-
concentrated in the United States (83%), with growing contributions from ing cause of ill health worldwide.[1] Further-
Europe, China, and Australia. Electrocorticography (ECoG)-based devices more, most individuals with SCI sustain
increasingly emerge alongside micro-electrode arrays. iBCI devices are now their injury before the age of 50, resulting in
being used to control a broader range of effectors, including robotic decades with increased dependence on care
and reduced quality of life.[2–4]
prosthetics and digital technologies. Although most (69.6%) studies reported
In recent decades, brain–computer inter-
outcome measures prospectively, these primarily related to decoding (69.6%) faces (BCIs) have emerged as a transforma-
and task performance (62.5%), with only 17.9% assessing clinical outcomes. tive technology to restore function by de-
When cassessed, clinical outcomes were highly heterogeneous due to varied coding preserved neural signals and trans-
approaches across target populations. iBCIs show potential to restore mitting this activity via computers to effec-
tor devices, enabling the performance of
functional independence at scale. However, challenges remain
desired actions. These prosthetic systems
around cross-subject generalization, scalable implantation, and outcome function by recording neural signals, de-
standardization. Novel measures should be developed collaboratively with coding the signals into desired output ac-
engineers, clinicians, and individuals with lived experience of motor tions, and executing these actions via an ef-
impairment. fector in the environment. Various systems
have been investigated to accomplish each
E. Dohle, S. Yusuf, J. Brannigan L. Jovanovic
Oxford University Hospitals East and North Hertfordshire NHS Trust
John Radcliffe Hospital Lister Hospital
Oxford OX3 9DU, UK Stevenage SG1 4AB, UK
E-mail: L. Thompson
E. Swanson Faculty of Medicine
Utrecht University Medical Centre Imperial College London
Utrecht 3584 CX, Netherlands London SW7 5NH, UK
H. L. Horsfall, W. Muirhead
Department of Neurosurgery
National Hospital for Neurology and Neurosurgery
The ORCID identification number(s) for the author(s) of this article London WC1N 3BG, UK
can be found under https://doi.org/10.1002/advs.202501912 H. L. Horsfall, W. Muirhead
The Francis Crick Institute
© 2025 The Author(s). Advanced Science published by Wiley-VCH
London NW1 1AT, UK
GmbH. This is an open access article under the terms of the Creative
Commons Attribution License, which permits use, distribution and H. L. Horsfall, W. Muirhead
reproduction in any medium, provided the original work is properly cited. Institute of Neurology
University College London
DOI: 10.1002/advs.202501912 London WC1N 3BG, UK
Adv. Sci. 2025, 12, e01912 e01912 (1 of 19) © 2025 The Author(s). Advanced Science published by Wiley-VCH GmbH
, 21983844, 2025, 32, Downloaded from https://advanced.onlinelibrary.wiley.com/doi/10.1002/advs.202501912 by Francis Crick Institute, Wiley Online Library on [04/09/2025]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
www.advancedsciencenews.com www.advancedscience.com
Figure 1. Example of experimental setup of an implantable brain–computer interface with a digital effector.
of these steps. Sensors may be implanted intracranially, such as sory feedback.[18,20–22] Although non-implantable BCI paradigms
micro-electrode arrays (MEAs), surface ECoG arrays, or endovas- using EEG have demonstrated clinical benefit,[23] and impor-
cular stent arrays. Alternatively, sensing may be non-implantable, tant progress has been made in enabling digital control,[24,25] ex-
using wearable device techniques like scalp electroencephalogra- tracranial electrical recording is limited by several factors. These
phy (EEG) and functional near-infrared spectroscopy (fNIRS).[5] include poor spatial discrimination, low-pass filtering in the
Decoding of neural signals may be performed using a vari- frequency domain resulting from the transmission of signals
ety of neural signal processing techniques. Outputs can drive through the skull, and the requirement for skin abrasion during
a range of effectors, including robotic prosthetic limbs,[6–8] vir- routine setup of extracranial sensors to enable clinically useable
tual avatars,[9–11] consumer digital devices,[12–15] and decoded recordings.
speech.[16–19] A typical BCI system with a digital device effector is Building on advances in implantable BCIs, there are numer-
shown in Figure 1. This is an example of an implantable system ous academic and commercial efforts to translate these systems
requiring a percutaneous connection, which has been commonly at scale and restore functional independence for individuals with
used in research settings to make seminal engineering and sci- motor impairments as part of routine clinical practice.[15,26] How-
entific advances in recent decades.[19,20] ever, no iBCI technology has yet received regulatory approval for
Implantable BCI (iBCI) systems have yielded significant clini- clinical use or been integrated into standard clinical practice. A
cal and engineering breakthroughs. This includes the first long- major challenge in the clinical translation of iBCI devices is the
term independent device use at home (in a controlled, clinical absence of consensus for clinically meaningful outcome mea-
trial setting), computer cursor control, high-dimensional pros- sures that can be used when evaluating device efficacy in clinical
thetic limb control, restoration of own muscle control via func- trials.[27,28] In the USA, the Food and Drug Administration has
tional electrical stimulation or spinal cord stimulation, high- highlighted the absence of an appropriate outcome measure[29]
speed communication output rates, and delivery of somatosen- and government funding has been awarded to investigate this.[30]
In this review, we present the largest and most up-to-date es-
timate of iBCI clinical trial participants worldwide, drawing on
data from 112 studies and integrating both published and veri-
L. Bashford fied unpublished sources. Unlike previous reviews that include
Bioscience Institute, Faculty of Medical Sciences
Newcastle University early-stage applications in contexts such as epilepsy,[31] the scope
Newcastle upon Tyne NE1 7RU, UK of our analysis is deliberately confined to clinical trials involv-
L. Bashford ing target populations with motor impairments, which includes
Department of Neurosurgery loss of limb function and/or speech. By focusing on individu-
University of Colorado als with ALS, SCI, and stroke, this review directly addresses the
Denver, CO 80045, USA
cohorts that stand to benefit most from the clinical translation
J. Brannigan
Department of Medical Physics and Biomedical Engineering
of iBCI technology. We establish a comprehensive registry not
University College London only as a new benchmark for assessing the global status of iBCI
London WC1E 6BT, UK trials, but also to serve as an essential resource for stakehold-
Adv. Sci. 2025, 12, e01912 e01912 (2 of 19) © 2025 The Author(s). Advanced Science published by Wiley-VCH GmbH
, 21983844, 2025, 32, Downloaded from https://advanced.onlinelibrary.wiley.com/doi/10.1002/advs.202501912 by Francis Crick Institute, Wiley Online Library on [04/09/2025]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
www.advancedsciencenews.com www.advancedscience.com
ers aiming to advance these technologies toward routine clinical Table 1. Exclusion criteria.
use.
To contextualize the field, we first map the evolution of iBCI Exclusion criteria
research trends, chronicling both the technical advances over 1 No use of implantable BCI devices
time and the heterogeneity in approaches that have contributed 2 Not a full text, independent publication
to the current challenges. We critically examine a key factor lim-
3 Not a primary study
iting clinical translation, namely the heterogeneity of outcome
4 Text not available in English
measures currently used to assess iBCI performance. We pro-
5 Full text not available
pose forward-looking solutions to the selection of appropriate
and standardized outcome measures, intending to extend the dis- 6 Non-human subjects
cussion to a multidisciplinary audience and accelerate the inte-
gration of iBCIs into standard clinical practice.
Cochlear implants were sensory prostheses which neither record
neural activity nor control external devices, and hence were not
included in this study.[36,37] Studies conducted in which there was
2. Experimental Section transient device implantation with a primary aim to aid peri-
This review was conducted in accordance with the pre- operative planning, for example, for seizure localization, were
ferred reporting items for systematic reviews and meta-analysis considered beyond the scope of this review. All full-text primary
(PRISMA) 2020 guidelines.[32] A completed checklist is included research papers in English were considered. Studies reporting
in the Materials SA (Supporting Information). This systematic exclusively on non-human subjects were excluded. An overview
review was prospectively registered on Open Science Framework of the exclusion hierarchy as provided to reviewers is shown in
(OSF) (https://osf.io/deyrj). Table 1.
2.4. Data Management, Extraction, and Appraisal
2.1. Search Strategy
Records were deduplicated using Rayyan.[38] Subsequently,
A sensitive search strategy was developed which combined syn-
records were blinded and screened by title and abstract by two in-
onyms for BCIs, intracortical, and patient, in consultation with
dependent reviewers. Full-text screening and data extraction were
a senior medical librarian. The search was applied to MEDLINE,
performed using a piloted data extraction proforma in MS Excel.
Embase and CINAHL using Ovid (Wolters Kluwer, Netherlands),
Risk of bias was assessed by two reviewers using the Mixed Meth-
and run from inception to 24th December 2024. The search strat-
ods Appraisal Tool checklist. Reference management was done
egy is included in Materials SB (Supporting Information). Fur-
using Zotero.
ther studies were identified through searching reference lists of
included records and searching the Google Scholar profiles of key
principal investigators in the field. 2.5. Data Synthesis
Analysis was performed in R (R Core Team, 2019) using the Tidy-
2.2. Study Selection verse package. As many participants were reported on in multiple
studies, the included studies were cross-referenced to match the
Included records were screened by two independent reviewers same participants across studies and prevent duplication of de-
(ED, ES). An initial pilot screen of 50 records was carried out to mographic details.[39] Plots were produced in R using the ggplot2
ensure concordance, following which reviewers were blinded to package.[40] Open-source R code shared in a previous publication
each other’s decisions using Rayyan (Rayyan Systems Inc, Cam- was adapted to create the map seen in Figure 2.[41] Graphics were
bridge, MA, USA). Disagreements were resolved by consensus produced using Inkscape (Inkscape Project, 2020).
or discussion with a third reviewer (JB). Full-text screening was Publications were grouped in 5-year intervals. Figures 3 and 4
carried out by the same reviewers (ED, ES). and 7, which show the proportions of different categories over
time, excluded time intervals with ≤3 published studies.
A subgroup analysis was carried out on studies which reported
2.3. Inclusion and Exclusion Criteria the use of iBCIs for communication purposes, either via cursor-
controlled typing or speech phoneme decoding paradigms. To
Studies were considered if they demonstrated the use of im- compare changes in achieved communication speed across stud-
plantable BCI devices with an intracranial sensing component ies over time, correct characters per minute (CCPM) estimates
and effector. For the purpose of this review, an implantable BCI were converted to words per minute (WPM) using the commonly
was defined as an intracranial device which records neural activ- used conversion factor of WPM = CPM/5. When speed was re-
ity representing volitional motor intent, such as intended limb ported in terms of characters per minute, it was combined with
movement or speech, and decoded this into an output signal to the reported error rate to calculate an estimate of correct charac-
control an external effector.[25] Non-implantable BCIs were pre- ters per minute. For each participant, the highest achieved mean
viously discussed in detail and had a limited potential to pro- speed was used, even if aided by additional technology, for exam-
vide clinically meaningful restoration of motor function.[5,33–35] ple, predictive typing or altered keyboard layouts. Accuracy was
Adv. Sci. 2025, 12, e01912 e01912 (3 of 19) © 2025 The Author(s). Advanced Science published by Wiley-VCH GmbH