Antidysrhythmic drugs
Chapter 26
Dysrhythmia
• Any deviation from the normal rhythm of the heart
Antidysrhythmic
• Used for the treatment and prevention of disturbances in cardiac rhythm
Action Potentials
• A change in the distribution of ions causes cardiac cells to become excited.
• The movement of ions across the cardiac cell’s membrane results in an
electrical impulse spreading across the cardiac cells.
• This electrical impulse leads to contraction
of the myocardial muscle.
• Four phases
- The sinoatrial node and the Purkinje cells each have separate action
potentials.
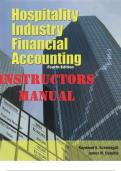
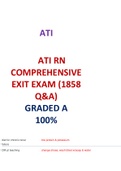
Electrocardiography
• Electrocardiogram (ECG or EKG)
• P wave
• PR interval
• QRS complex
• ST segment
• T wave
,Common dysrhythmias: Vaughan Williams Classification
• Supraventricular dysrhythmias • System commonly used to classify antidysrhythmic drugs
• Ventricular dysrhythmias • Based on the electrophysiological effect of particular drugs
• Ectopic foci on the action potential
• Conduction blocks • Class I
- Class Ia
- Class Ib
- Class Ic
• Class II
• Class III
• Class IV
Class I Class Ia Class Ib Class II
Membrane-stabilizing Procainamide, quinidine, and Lidocaine hydrochloride ß-blockers
drugs disopyramide (Xylocaine®) Reduce or block sympathetic
Fast sodium channel Block sodium (fast) channels Block sodium channels nervous system stimulation, thus
blockers Delay repolarization Accelerate repolarization reducing transmission of impulses
Divided into Ia, Ib, and Increase action potential Increase or decrease APD in the heart’s conduction system
Ic drugs, according duration (APD) Lidocaine is used for ventricular Depress phase 4 depolarization
to effects Used for atrial fibrillation, dysrhythmias only. General myocardial depressants for
premature atrial contractions, Phenytoin is used for atrial and both supraventricular and
premature ventricular ventricular tachydysrhythmias ventricular dysrhythmias
contractions, ventricular caused by digitalis toxicity or long Also used as antianginal and
tachycardia QT syndrome. antihypertensive drugs
Action: raises the ventricular Atenolol:
fibrillation threshold Cardioselective ß-blocker;
Significant adverse effects on the preferentially blocks the ß1-
central nervous system (CNS): adrenergic receptors that are
twitching, convulsions, confusion, located primarily in the heart.
respiratory depression or arrest, Noncardioselective ß-blockers
hypotension, bradycardia, and block not only the ß1-adrenergic
dysrhythmias receptors in the heart but also the
, Contraindications: ß2-adrenergic receptors in the lungs
hypersensitive, severe sinoatrial and therefore can exacerbate pre-
or atrioventricular existing asthma or chronic
intraventricular block, or Stokes- obstructive pulmonary disease.
Adams or Wolff-Parkinson-White Uses: antidysrhythmic,
syndrome hypertension, and angina
Contraindications: severe
bradycardia, second- or third-
degree heart block, heart failure,
cardiogenic shock, or a known
hypersensitivity
Class III Class IV Unclassified
Amiodarone, dronedarone, sotalol, ibutilide Calcium channel blockers Adenosine (Adenocard®)
Increase APD - Inhibit slow channel (calcium- - Slows conduction through the
Prolong repolarization in phase 3 dependent) pathways atrioventricular node
Used for dysrhythmias that are difficult to Depress phase 4 depolarization - Used to convert PSVT to sinus
treat Reduce atrioventricular node conduction rhythm
Life-threatening ventricular tachycardia or Used for paroxysmal supraventricular - Very short half-life—less than 10
fibrillation, atrial fibrillation or flutter that is tachycardia (PSVT); rate control for atrial seconds
resistant to other drugs fibrillation and flutter - Only administered as fast
Amiodarone: Diltiazem: intravenous (IV) push
Markedly prolongs the action potential Temporary control of a rapid ventricular - May cause asystole for a few
duration and the effective refractory period response in patients with atrial fibrillation or seconds
in all cardiac tissues flutter and PSVT - Other adverse effects are
Blocks both the α- and ß-adrenergic Contraindications: hypersensitivity, acute minimal.
receptors of the sympathetic nervous system myocardial infarction, pulmonary congestion,
Uses: one of the most effective Wolff-Parkinson-White syndrome, severe
antidysrhythmic drugs for controlling hypotension, cardiogenic shock, sick sinus
supraventricular and ventricular syndrome, or second- or third-degree AV
dysrhythmias block
, Drug of choice for ventricular dysrhythmias
according to the Advanced Cardiac Life
Support guidelines
Most serious effect: pulmonary toxicity
Other adverse effects: corneal
microdeposits, which may cause visual halos,
photophobia, and dry eyes; photosensitivity;
and pulmonary toxicity
Drug interactions: digoxin and warfarin
sodium
Contraindications: hypersensitivity, severe
sinus bradycardia or second- or third-degree
heart block
Antidysrhythmic Interactions:
Warfarin sodium (Coumadin®): monitor international normalized ratio (INR)
Grapefruit juice: amiodarone, disopyramide, and quinidine
Adverse effects:
All antidysrhythmics can cause dysrhythmias!
• Hypersensitivity reactions
• Nausea, vomiting, and diarrhea
• Dizziness
• Headache, and blurred vision
• Prolongation of the QT interval
Contraindications:
Known drug allergy
Second- or third-degree atrioventricular block, bundle branch block, cardiogenic shock, sick sinus syndrome, and
any other ECG changes, depending on the clinical judgment of a cardiologist.
Other antidysrhythmic drugs
Nursing Implications:
• During therapy, monitor cardiac rhythm, heart rate, blood pressure, general well-being, skin colour, temperature,
and heart and lung sounds.
Chapter 26
Dysrhythmia
• Any deviation from the normal rhythm of the heart
Antidysrhythmic
• Used for the treatment and prevention of disturbances in cardiac rhythm
Action Potentials
• A change in the distribution of ions causes cardiac cells to become excited.
• The movement of ions across the cardiac cell’s membrane results in an
electrical impulse spreading across the cardiac cells.
• This electrical impulse leads to contraction
of the myocardial muscle.
• Four phases
- The sinoatrial node and the Purkinje cells each have separate action
potentials.
Electrocardiography
• Electrocardiogram (ECG or EKG)
• P wave
• PR interval
• QRS complex
• ST segment
• T wave
,Common dysrhythmias: Vaughan Williams Classification
• Supraventricular dysrhythmias • System commonly used to classify antidysrhythmic drugs
• Ventricular dysrhythmias • Based on the electrophysiological effect of particular drugs
• Ectopic foci on the action potential
• Conduction blocks • Class I
- Class Ia
- Class Ib
- Class Ic
• Class II
• Class III
• Class IV
Class I Class Ia Class Ib Class II
Membrane-stabilizing Procainamide, quinidine, and Lidocaine hydrochloride ß-blockers
drugs disopyramide (Xylocaine®) Reduce or block sympathetic
Fast sodium channel Block sodium (fast) channels Block sodium channels nervous system stimulation, thus
blockers Delay repolarization Accelerate repolarization reducing transmission of impulses
Divided into Ia, Ib, and Increase action potential Increase or decrease APD in the heart’s conduction system
Ic drugs, according duration (APD) Lidocaine is used for ventricular Depress phase 4 depolarization
to effects Used for atrial fibrillation, dysrhythmias only. General myocardial depressants for
premature atrial contractions, Phenytoin is used for atrial and both supraventricular and
premature ventricular ventricular tachydysrhythmias ventricular dysrhythmias
contractions, ventricular caused by digitalis toxicity or long Also used as antianginal and
tachycardia QT syndrome. antihypertensive drugs
Action: raises the ventricular Atenolol:
fibrillation threshold Cardioselective ß-blocker;
Significant adverse effects on the preferentially blocks the ß1-
central nervous system (CNS): adrenergic receptors that are
twitching, convulsions, confusion, located primarily in the heart.
respiratory depression or arrest, Noncardioselective ß-blockers
hypotension, bradycardia, and block not only the ß1-adrenergic
dysrhythmias receptors in the heart but also the
, Contraindications: ß2-adrenergic receptors in the lungs
hypersensitive, severe sinoatrial and therefore can exacerbate pre-
or atrioventricular existing asthma or chronic
intraventricular block, or Stokes- obstructive pulmonary disease.
Adams or Wolff-Parkinson-White Uses: antidysrhythmic,
syndrome hypertension, and angina
Contraindications: severe
bradycardia, second- or third-
degree heart block, heart failure,
cardiogenic shock, or a known
hypersensitivity
Class III Class IV Unclassified
Amiodarone, dronedarone, sotalol, ibutilide Calcium channel blockers Adenosine (Adenocard®)
Increase APD - Inhibit slow channel (calcium- - Slows conduction through the
Prolong repolarization in phase 3 dependent) pathways atrioventricular node
Used for dysrhythmias that are difficult to Depress phase 4 depolarization - Used to convert PSVT to sinus
treat Reduce atrioventricular node conduction rhythm
Life-threatening ventricular tachycardia or Used for paroxysmal supraventricular - Very short half-life—less than 10
fibrillation, atrial fibrillation or flutter that is tachycardia (PSVT); rate control for atrial seconds
resistant to other drugs fibrillation and flutter - Only administered as fast
Amiodarone: Diltiazem: intravenous (IV) push
Markedly prolongs the action potential Temporary control of a rapid ventricular - May cause asystole for a few
duration and the effective refractory period response in patients with atrial fibrillation or seconds
in all cardiac tissues flutter and PSVT - Other adverse effects are
Blocks both the α- and ß-adrenergic Contraindications: hypersensitivity, acute minimal.
receptors of the sympathetic nervous system myocardial infarction, pulmonary congestion,
Uses: one of the most effective Wolff-Parkinson-White syndrome, severe
antidysrhythmic drugs for controlling hypotension, cardiogenic shock, sick sinus
supraventricular and ventricular syndrome, or second- or third-degree AV
dysrhythmias block
, Drug of choice for ventricular dysrhythmias
according to the Advanced Cardiac Life
Support guidelines
Most serious effect: pulmonary toxicity
Other adverse effects: corneal
microdeposits, which may cause visual halos,
photophobia, and dry eyes; photosensitivity;
and pulmonary toxicity
Drug interactions: digoxin and warfarin
sodium
Contraindications: hypersensitivity, severe
sinus bradycardia or second- or third-degree
heart block
Antidysrhythmic Interactions:
Warfarin sodium (Coumadin®): monitor international normalized ratio (INR)
Grapefruit juice: amiodarone, disopyramide, and quinidine
Adverse effects:
All antidysrhythmics can cause dysrhythmias!
• Hypersensitivity reactions
• Nausea, vomiting, and diarrhea
• Dizziness
• Headache, and blurred vision
• Prolongation of the QT interval
Contraindications:
Known drug allergy
Second- or third-degree atrioventricular block, bundle branch block, cardiogenic shock, sick sinus syndrome, and
any other ECG changes, depending on the clinical judgment of a cardiologist.
Other antidysrhythmic drugs
Nursing Implications:
• During therapy, monitor cardiac rhythm, heart rate, blood pressure, general well-being, skin colour, temperature,
and heart and lung sounds.