Med Surg 2 Tanasha C.Matta
Exam 2 Review
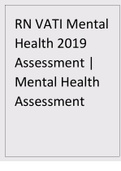
Heart Sounds & Their Location
Auscultate in a systemic order, Think “APE To Man”;
• Aortic
• Pulmonary
• ERBs point
• Tricuspid
• Mitral
- Aortic Valve: 2nd intercostal space on the RIGHT of the sternum
- Pulmonary Valve: 2nd intercostal space on the LEFT of the sternum
- Tricuspid Valve: 5th intercostal space at the LEFT LOWER sternal border
- Mitral Valve: 5th intercostal space at the APEX of the heart.
Normal Heart Sounds
- S1: Closure of Mitral and Tricuspid Valve. It is a low pitch and is best heard at the lower left
sternal border or the APEX of the heart.
- S2: Closing of the Aortic and Pulmonic Valves (semilunar valves). It is a higher pitch and is
heard best at the base of the heart at the END of ventricular systole.
Abnormal Heart Sounds
- S3: (Ventricular Gallop), Most likely to be a normal finding in those younger than 35 years. An
S3 gallop in older pts is abnormal and represent a decrease in left ventricular compliance. It
can be detected as an early sign of heart failure or as a ventricular septal defect.
- S4: (Atrial Gallop), May be heard in pts with hypertension, anemia, hypertrophy, myocardial
infarction, aortic or pulmonic stenosis, and pulmonary emboli. It may also be heard with
advancing age due to a stiffened ventricle.
- Murmurs: Reflect turbulent blood flow through normal or abnormal valves. They are classified
according to their timing in the cardiac cycle: Systolic murmur occurs between S1 and S2,
Diastolic murmur occurs between S2 and S1. Describe the location based on where they are
best heard. Some murmurs transmit or radiate from their loudest point to other areas,
including neck, back and the axilla. The configuration is described as crescendo (increases in
intensity) or decrescendo (decrease in intensity). Can be further characterized as harsh,
blowing, whistling, rumbling or squeaking and are described by pitch, high or low.
- Pericardial Friction Rub: Rubs are usually transient and are a sign of inflammation, infection,
or infiltration. They may be heard in pts with pericarditis resulting from MI or cardiac
tamponade or after thoracotomy.
Cardiac Assessment
Cardiac Output = Heart rate x Stroke volume (the number of times the ventricles contract per min x
the amount of blood ejected by the left ventricle during each contraction.)
Tachycardia: Heart rate >100 BPM
Bradycardia: Heart rate <60 BPM
Pulse Locations: Carotid, Femoral, Radial, Popliteal,
Capillary refill time: Less than 2 sec
Cardiovascular Lab Profile
- Serum Lipids
§ Cholesterol: <200 mg/dL – Elevations indicate increased risk for CAD
§ Triglycerides: Females; 35-135, Males; 40-160 mg/dL – Elevations indicate
increased risk for CAD
, § HDLs: Females; >55, Males; >45 mg/dL – Elevations protect against CAD
§ LDLs; <130 mg/dL – Elevations indicate increased risk for CAD
§ CRP; <1.0 mg/dL– Elevations may indicate tissue infarction or damage
- Serum Markers
§ Troponin T; <0.1 ng/mL – Elevations indicate MI
§ Troponin I; <0.03 ng/mL – Elevations indicate MI
Atherosclerosis
Buildup of fats, cholesterol and other substances in or on the walls of the ARTERY and is the leading
risk factor for cardiovascular disease (CVD).
- Assess pt BP in both arms as well as all pulse sites, check temperature difference in lower
extremities. Check capillary filling. Prolonged capillary filling (>3 secs in young to middle-aged
adults, >5 secs in older adults). Many pts with vascular disease have a bruit in the larger
arteries.
Bruit: a turbulent, swishing sound which can be a soft or loud pitch, often occurring in the carotid,
aortic, femoral, & popliteal arteries.
Critical Rescue: A decrease in intensity or a complete loss of a pulse in a pt with atherosclerosis may
indicate an arterial occlusion (blockage) in the area supplied by the artery. If pulse is not palpable, use a
doppler to further assess pulse. Immediately report to HCP and document for emergency
management.
- Risk Factors: Low HDL, High LDL, Increased Triglycerides, Genetics, Diabetes mellitus, Obesity,
Hypertension, Sedentary lifestyle, Smoking, Stress, Black or Hispanic race/ethnicity, Older
adult, Diet high in saturated and trans-fat/cholesterol/sodium & sugar.
- S|S: Cool extremities, Bruits, Chest discomfort during exercise or stress, Leg cramps when
walking, & SOB with minimal activity.
- Dx testing: Lipid Panel
• Total Cholesterol: <200
• LDL: <130 “BAD cholesterol”
• HDL: >45 in Males, >55 in Females “GOOD cholesterol”
• Triglycerides: <150
- Drug Therapy: “Statins” used to reduce overall cholesterol. Lovastatin, Atorvastatin,
Simvastatin, etc. Contraindication: Pts with Liver disease, and Women of Child baring age. Pts
should avoid grapefruit juice with these meds. Potential interaction with warfarin, cyclosporin,
and selected antibiotics. Pt teaching: reduce calories & saturated fat, trans fat, and cholesterol
should be limited. Pts should consume low-fat dairy product, fruits, vegetables, and whole
grains.
Cardiovascular Disease Risk Factors
- Smoking
- Obesity
- Diabetes
Cardiac Tamponade **EMERGENCY**
Acute cardiac tamponade may occur when small volumes (20-50 mL) of fluid accumulate rapidly in the
pericardium and causes a sudden decrease in cardiac output. Cardiac tamponade can occur with
pericarditis, as well as other conditions such as ventricular wall rupture from acute MI, cancer, and
aortic dissection and as a complication from invasive procedures. Report any suspicion of this
complication to the HCP immediately!!
- Findings; JVD, PARADOXICAL PULSE, Tachycardia, MUFFLED HEART SOUNDS, Hypotension.
- Intervention; Initially managed the decreased CO with increased fluid volume administration
while awaiting Echocardiogram or Xray to confirm dx. The HCP may elect to perform
PERICARDIOCENTESIS to remove fluid and relieve the pressure on the heart. After
Exam 2 Review
Heart Sounds & Their Location
Auscultate in a systemic order, Think “APE To Man”;
• Aortic
• Pulmonary
• ERBs point
• Tricuspid
• Mitral
- Aortic Valve: 2nd intercostal space on the RIGHT of the sternum
- Pulmonary Valve: 2nd intercostal space on the LEFT of the sternum
- Tricuspid Valve: 5th intercostal space at the LEFT LOWER sternal border
- Mitral Valve: 5th intercostal space at the APEX of the heart.
Normal Heart Sounds
- S1: Closure of Mitral and Tricuspid Valve. It is a low pitch and is best heard at the lower left
sternal border or the APEX of the heart.
- S2: Closing of the Aortic and Pulmonic Valves (semilunar valves). It is a higher pitch and is
heard best at the base of the heart at the END of ventricular systole.
Abnormal Heart Sounds
- S3: (Ventricular Gallop), Most likely to be a normal finding in those younger than 35 years. An
S3 gallop in older pts is abnormal and represent a decrease in left ventricular compliance. It
can be detected as an early sign of heart failure or as a ventricular septal defect.
- S4: (Atrial Gallop), May be heard in pts with hypertension, anemia, hypertrophy, myocardial
infarction, aortic or pulmonic stenosis, and pulmonary emboli. It may also be heard with
advancing age due to a stiffened ventricle.
- Murmurs: Reflect turbulent blood flow through normal or abnormal valves. They are classified
according to their timing in the cardiac cycle: Systolic murmur occurs between S1 and S2,
Diastolic murmur occurs between S2 and S1. Describe the location based on where they are
best heard. Some murmurs transmit or radiate from their loudest point to other areas,
including neck, back and the axilla. The configuration is described as crescendo (increases in
intensity) or decrescendo (decrease in intensity). Can be further characterized as harsh,
blowing, whistling, rumbling or squeaking and are described by pitch, high or low.
- Pericardial Friction Rub: Rubs are usually transient and are a sign of inflammation, infection,
or infiltration. They may be heard in pts with pericarditis resulting from MI or cardiac
tamponade or after thoracotomy.
Cardiac Assessment
Cardiac Output = Heart rate x Stroke volume (the number of times the ventricles contract per min x
the amount of blood ejected by the left ventricle during each contraction.)
Tachycardia: Heart rate >100 BPM
Bradycardia: Heart rate <60 BPM
Pulse Locations: Carotid, Femoral, Radial, Popliteal,
Capillary refill time: Less than 2 sec
Cardiovascular Lab Profile
- Serum Lipids
§ Cholesterol: <200 mg/dL – Elevations indicate increased risk for CAD
§ Triglycerides: Females; 35-135, Males; 40-160 mg/dL – Elevations indicate
increased risk for CAD
, § HDLs: Females; >55, Males; >45 mg/dL – Elevations protect against CAD
§ LDLs; <130 mg/dL – Elevations indicate increased risk for CAD
§ CRP; <1.0 mg/dL– Elevations may indicate tissue infarction or damage
- Serum Markers
§ Troponin T; <0.1 ng/mL – Elevations indicate MI
§ Troponin I; <0.03 ng/mL – Elevations indicate MI
Atherosclerosis
Buildup of fats, cholesterol and other substances in or on the walls of the ARTERY and is the leading
risk factor for cardiovascular disease (CVD).
- Assess pt BP in both arms as well as all pulse sites, check temperature difference in lower
extremities. Check capillary filling. Prolonged capillary filling (>3 secs in young to middle-aged
adults, >5 secs in older adults). Many pts with vascular disease have a bruit in the larger
arteries.
Bruit: a turbulent, swishing sound which can be a soft or loud pitch, often occurring in the carotid,
aortic, femoral, & popliteal arteries.
Critical Rescue: A decrease in intensity or a complete loss of a pulse in a pt with atherosclerosis may
indicate an arterial occlusion (blockage) in the area supplied by the artery. If pulse is not palpable, use a
doppler to further assess pulse. Immediately report to HCP and document for emergency
management.
- Risk Factors: Low HDL, High LDL, Increased Triglycerides, Genetics, Diabetes mellitus, Obesity,
Hypertension, Sedentary lifestyle, Smoking, Stress, Black or Hispanic race/ethnicity, Older
adult, Diet high in saturated and trans-fat/cholesterol/sodium & sugar.
- S|S: Cool extremities, Bruits, Chest discomfort during exercise or stress, Leg cramps when
walking, & SOB with minimal activity.
- Dx testing: Lipid Panel
• Total Cholesterol: <200
• LDL: <130 “BAD cholesterol”
• HDL: >45 in Males, >55 in Females “GOOD cholesterol”
• Triglycerides: <150
- Drug Therapy: “Statins” used to reduce overall cholesterol. Lovastatin, Atorvastatin,
Simvastatin, etc. Contraindication: Pts with Liver disease, and Women of Child baring age. Pts
should avoid grapefruit juice with these meds. Potential interaction with warfarin, cyclosporin,
and selected antibiotics. Pt teaching: reduce calories & saturated fat, trans fat, and cholesterol
should be limited. Pts should consume low-fat dairy product, fruits, vegetables, and whole
grains.
Cardiovascular Disease Risk Factors
- Smoking
- Obesity
- Diabetes
Cardiac Tamponade **EMERGENCY**
Acute cardiac tamponade may occur when small volumes (20-50 mL) of fluid accumulate rapidly in the
pericardium and causes a sudden decrease in cardiac output. Cardiac tamponade can occur with
pericarditis, as well as other conditions such as ventricular wall rupture from acute MI, cancer, and
aortic dissection and as a complication from invasive procedures. Report any suspicion of this
complication to the HCP immediately!!
- Findings; JVD, PARADOXICAL PULSE, Tachycardia, MUFFLED HEART SOUNDS, Hypotension.
- Intervention; Initially managed the decreased CO with increased fluid volume administration
while awaiting Echocardiogram or Xray to confirm dx. The HCP may elect to perform
PERICARDIOCENTESIS to remove fluid and relieve the pressure on the heart. After