Week 10: Neuroimaging
MRI contrast
THE MR image does not exist → an unlimited number of variations are possible.
The basis: PD (proton density) = always present in every MRI.
MRI basis:
● T1 and T2 refer to the time between the magnetic pulse and the image taken. These
differences are used to detect different structures on the MRI. They are tissue
properties.
○ T1: fat = light, water = dark.
○ T2: water tissues appear lighter compared to fat tissues. Suppose the grey
matter is lighter than the white matter → T2.
● The most important choices are TE and TR
○ TR: repetition time: short TR gives better T1
○ TE: echo time: long TE gives better T2
Basis of no questions asked, just for understanding
● Signal and image formation: put a patient into a big magnet. The protons (H+) align
with the magnetic field.
● When you apply radio waves (RF pulse) at a good frequency you can change the
orientation of the spins as they absorb energy. After you turn the radio waves off,
they return to equilibrium.
Contrast formation:
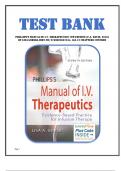
● MRI creates a magnetic field, forcing the H+ to align with eachother (picture on the
left). Then, there there is an RF causing the H+ to align against their gradient
(picture on the right). After this citation, the H+ moves back to equilibirium. This
takes different time between the tissues, and that is what you measure.
○ Relaxation of longitudinal component → Mz → M0 = T1 = spin-lattice
○ Relaxation of transverse component → Mxz → 0 = T2 = spin-spin
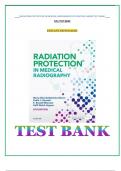
○ T1 relaxation: LOG increasing curve at different spinning points. Contrast =
(Mz-Mz) of T1 of different tissues. Saturation spins at t=0. At some point,
there is a maximum difference of contrast. Relaxation time:
, ○ T2 relaxation: LOG decreasing at different
spinning points. Excitation spins at t=0. With an
Contrast versus TR & TE: increasing echo time, there is an increasing
contrast difference.
When do you use which contrast:
T1 weighted T2 weighted PD weighted
anatomy, good SNR/unit pathology anatomy/MS lesions
time
additional information tumour, oedema, lesions additional information
pathology (MS) pathology.
Spin-echo/gradient echo:
● Gradient echo (GRE) = T2* contrast = T2 + the effect of the local perturbation of the
magnetic field. This T2* depends on TE
○ Micro-bleeds (iron or calcium) can be seen in gradient echo, T2* weighted.
● Spin echo (SE) or Hahn-echo = refocus macroscopical dephasing. Only spin echo
can provide real T2 contrast. The amount of T2 depends on TE.
Magnetisation preparation pulses:
● We can work with contrast manipulation. Fluid attenuated inversion recovery =
FLAIR.
○ FLAIR = removes the signal of CSF by suppression, resulting in a T2 image
with dark CSF.
○ This is used to identify MS lesions.
● Contrast agents: used to create a better MRI picture.
○ Results in a reduction of T1 and T2 of the water protons → the contrast agent
itself does not produce the MR signal.
■ A shortening of T1 → signal enhancement.
■ High concentration of contrast agent → signal reduction in T2
shortening.
○ Shortening of the T1 →increase the signal of T1-weighted images. Often
used are Gd, Mn ions and iron particles.
, ■ Gd-DTPA molecule: Gd itself is toxic, but the DTPA shell makes it not
toxic to the body. IV injection. Extracellular agent. No BBB passage.
90 min T1/2.
Diffusion MRI
Basics:
● Brownian motion = the random movement of particles in the fluid.
● Factors that influence: temperature and viscosity.
● The diffusion coefficient also depends on the surrounding molecules.
○ Water in a liquid environment (like CSF) → have free diffusion.
○ Water in tissue → diffusion is hindered → smaller diffusion coefficient. At the
same time → smaller distance.
● Diffusion sensitising gradients = short additional magnetic field, varying with the
position.
○ Fixed water molecules = spin feel the same magnetic field, no effect of
gradients.
○ Mobiele water molecules = diffusing through CSF or extracellular space.
Spins feel different fields, resulting in loss of signal. The loss is larger when
the diffusion is faster and when the gradients are stronger.
○ B-value = the strength of diffusion weighting.
○ The apparent diffusion coefficient (ADC) = magnitude of diffusion of water
molecules inside the tissue.
○ DWI = measuring Brownian motion of water molecules within a tissue or
voxel.
○ Occlusion of artery --> high signal on DWI and low on ADC --> faillure of the
Na/K pump --> cell swelling --> cytoktoxi oedema --> restricted diffusion.
■ With an increasing b-value → decreasing ADC
■ ADC changes during development.
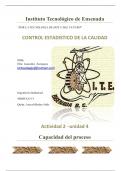
● Traveling along/parallel to axons is also called L1 or
axial diffusion → longitudinal along the optic nerve for
example. (D//).
● Strongly hindered perpendicular to nerve direction,
also called L23 or radial diffusivity → transverse
sections of the optic nerve. (D|).
● D (diffusion) is a tensor; you need at least 6 gradient directions to estimate D.
● Echo-planer imaging (EPI) = fast sequence, with a short TE as possible and always
T2 weighted.
● FA = 0 means isoptic = equally
restricted to all directions.
, FA is a measure of WM integrity:
FA = fractional anisotropy. Used to measure connectivity in the brain. Can be derived from
DTI.
● In MS there is demyelination → in the lesion there is a decreased FA.
● An increase of FA → better WM integrity.
● Colouring the FA can indicate the direction.
● Can be combined with a V1→ vector along where the diffusion is the highest.
● Dark bands in healthy volunteers → FA lower in WM → crossing fibres
Tractography = nerve tracts can be visualised using diffusion. This is only the possibility of a
direction.
● Clinical application: when the tumour is pressing the healthy tissue aside, you can
determine the tract. Possible to follow the healthy tissue.
○ Main motor fibres.
Neuroradiology
Computed tomography: CT
Pros:
● Fast (1 min), available 47/7
● God contrast for bone/air/CSF/fat/blood/calcification
● Easy to detect haemorrhage, fractures, ischemia.
○ Modality of choice in the acute setting especially trauma and stroke.
Cons:
● X-ray exposure
● Low diagnostic accuracy detection of small lesions
● Not very useful for characterization of brain lesions
● Beam-hardening artefacts = edges of an object to appear brighter than the centre,
even if the material is the same. → skull base and posterior fossa.
Houndsfield units (HU) = scaling of attenuation of various tissues/materials.
● Water = 0 by definition
● Bone = >1000
● Iodine contrast = 50-150
● Gray matter = 37
● White matter 32
● Fat = - 40
● Air = - 1000 by definition
● Hypodens: appear darker on a CT. Like air, fat, and water
● Hyperdens: appear lighter on a CT. Like blood, calcification and IV contrast
○ Contrast enhancement in
CT: intravenous iodinated
contrast (thicken the blood)
(hyperdense).
○ Enhance visibility/
discrimination in vascular
structures, tumours and
infections.
MRI contrast
THE MR image does not exist → an unlimited number of variations are possible.
The basis: PD (proton density) = always present in every MRI.
MRI basis:
● T1 and T2 refer to the time between the magnetic pulse and the image taken. These
differences are used to detect different structures on the MRI. They are tissue
properties.
○ T1: fat = light, water = dark.
○ T2: water tissues appear lighter compared to fat tissues. Suppose the grey
matter is lighter than the white matter → T2.
● The most important choices are TE and TR
○ TR: repetition time: short TR gives better T1
○ TE: echo time: long TE gives better T2
Basis of no questions asked, just for understanding
● Signal and image formation: put a patient into a big magnet. The protons (H+) align
with the magnetic field.
● When you apply radio waves (RF pulse) at a good frequency you can change the
orientation of the spins as they absorb energy. After you turn the radio waves off,
they return to equilibrium.
Contrast formation:
● MRI creates a magnetic field, forcing the H+ to align with eachother (picture on the
left). Then, there there is an RF causing the H+ to align against their gradient
(picture on the right). After this citation, the H+ moves back to equilibirium. This
takes different time between the tissues, and that is what you measure.
○ Relaxation of longitudinal component → Mz → M0 = T1 = spin-lattice
○ Relaxation of transverse component → Mxz → 0 = T2 = spin-spin
○ T1 relaxation: LOG increasing curve at different spinning points. Contrast =
(Mz-Mz) of T1 of different tissues. Saturation spins at t=0. At some point,
there is a maximum difference of contrast. Relaxation time:
, ○ T2 relaxation: LOG decreasing at different
spinning points. Excitation spins at t=0. With an
Contrast versus TR & TE: increasing echo time, there is an increasing
contrast difference.
When do you use which contrast:
T1 weighted T2 weighted PD weighted
anatomy, good SNR/unit pathology anatomy/MS lesions
time
additional information tumour, oedema, lesions additional information
pathology (MS) pathology.
Spin-echo/gradient echo:
● Gradient echo (GRE) = T2* contrast = T2 + the effect of the local perturbation of the
magnetic field. This T2* depends on TE
○ Micro-bleeds (iron or calcium) can be seen in gradient echo, T2* weighted.
● Spin echo (SE) or Hahn-echo = refocus macroscopical dephasing. Only spin echo
can provide real T2 contrast. The amount of T2 depends on TE.
Magnetisation preparation pulses:
● We can work with contrast manipulation. Fluid attenuated inversion recovery =
FLAIR.
○ FLAIR = removes the signal of CSF by suppression, resulting in a T2 image
with dark CSF.
○ This is used to identify MS lesions.
● Contrast agents: used to create a better MRI picture.
○ Results in a reduction of T1 and T2 of the water protons → the contrast agent
itself does not produce the MR signal.
■ A shortening of T1 → signal enhancement.
■ High concentration of contrast agent → signal reduction in T2
shortening.
○ Shortening of the T1 →increase the signal of T1-weighted images. Often
used are Gd, Mn ions and iron particles.
, ■ Gd-DTPA molecule: Gd itself is toxic, but the DTPA shell makes it not
toxic to the body. IV injection. Extracellular agent. No BBB passage.
90 min T1/2.
Diffusion MRI
Basics:
● Brownian motion = the random movement of particles in the fluid.
● Factors that influence: temperature and viscosity.
● The diffusion coefficient also depends on the surrounding molecules.
○ Water in a liquid environment (like CSF) → have free diffusion.
○ Water in tissue → diffusion is hindered → smaller diffusion coefficient. At the
same time → smaller distance.
● Diffusion sensitising gradients = short additional magnetic field, varying with the
position.
○ Fixed water molecules = spin feel the same magnetic field, no effect of
gradients.
○ Mobiele water molecules = diffusing through CSF or extracellular space.
Spins feel different fields, resulting in loss of signal. The loss is larger when
the diffusion is faster and when the gradients are stronger.
○ B-value = the strength of diffusion weighting.
○ The apparent diffusion coefficient (ADC) = magnitude of diffusion of water
molecules inside the tissue.
○ DWI = measuring Brownian motion of water molecules within a tissue or
voxel.
○ Occlusion of artery --> high signal on DWI and low on ADC --> faillure of the
Na/K pump --> cell swelling --> cytoktoxi oedema --> restricted diffusion.
■ With an increasing b-value → decreasing ADC
■ ADC changes during development.
● Traveling along/parallel to axons is also called L1 or
axial diffusion → longitudinal along the optic nerve for
example. (D//).
● Strongly hindered perpendicular to nerve direction,
also called L23 or radial diffusivity → transverse
sections of the optic nerve. (D|).
● D (diffusion) is a tensor; you need at least 6 gradient directions to estimate D.
● Echo-planer imaging (EPI) = fast sequence, with a short TE as possible and always
T2 weighted.
● FA = 0 means isoptic = equally
restricted to all directions.
, FA is a measure of WM integrity:
FA = fractional anisotropy. Used to measure connectivity in the brain. Can be derived from
DTI.
● In MS there is demyelination → in the lesion there is a decreased FA.
● An increase of FA → better WM integrity.
● Colouring the FA can indicate the direction.
● Can be combined with a V1→ vector along where the diffusion is the highest.
● Dark bands in healthy volunteers → FA lower in WM → crossing fibres
Tractography = nerve tracts can be visualised using diffusion. This is only the possibility of a
direction.
● Clinical application: when the tumour is pressing the healthy tissue aside, you can
determine the tract. Possible to follow the healthy tissue.
○ Main motor fibres.
Neuroradiology
Computed tomography: CT
Pros:
● Fast (1 min), available 47/7
● God contrast for bone/air/CSF/fat/blood/calcification
● Easy to detect haemorrhage, fractures, ischemia.
○ Modality of choice in the acute setting especially trauma and stroke.
Cons:
● X-ray exposure
● Low diagnostic accuracy detection of small lesions
● Not very useful for characterization of brain lesions
● Beam-hardening artefacts = edges of an object to appear brighter than the centre,
even if the material is the same. → skull base and posterior fossa.
Houndsfield units (HU) = scaling of attenuation of various tissues/materials.
● Water = 0 by definition
● Bone = >1000
● Iodine contrast = 50-150
● Gray matter = 37
● White matter 32
● Fat = - 40
● Air = - 1000 by definition
● Hypodens: appear darker on a CT. Like air, fat, and water
● Hyperdens: appear lighter on a CT. Like blood, calcification and IV contrast
○ Contrast enhancement in
CT: intravenous iodinated
contrast (thicken the blood)
(hyperdense).
○ Enhance visibility/
discrimination in vascular
structures, tumours and
infections.