Molecular Toxicology
This book was obligatory for this course, and it was used to make this summary:
Boelsterli, U. A. (2007). Mechanistic Toxicology: The Molecular Basis of How Chemicals Disrupt
Biological Targets (2nd ed.). CRC Press. https://doi.org/10.1201/9780367806293
Introduction lecture Chapter 1 & 2
Molecular toxicology and mechanisms of toxicity are required to:
- Estimate risk of human toxicity after exposure to a potentially toxic compound
- Determine toxicity thresholds
- Develop antidotes against acute toxicity
- Development of safe pharmaceuticals
- Develop biomarkers for exposure or toxicity
What is needed for toxicity
- Too high exposure
- Interaction with essential target
- Lack of cell adaptation to the stimulus
Paracelsus’ philosophy: “all compounds are poisons, but it’s the dose that determines if
something is toxic” too much of anything is never good
Dose (+ intrinsic properties) of a compound determine toxicity
- LD50 -> lethal dose (after which an animal is diseased within 50% of exposed animals)
- Potency of a compound has to do with the target it interferes with, and the mechanism
Route of exposure determines toxicity
- Ricin, when administrerd orally, has a di]erent LD50 (need higher dose) then when
injected directly
- Has to do with first pass metabolism and absorption in the intestines
(Internal) exposure determines toxicity -> “all substances are poisons, it is the exposure (of the
target) that determines if a substance is toxic or not”
Toxicokinetic factors; what does the body do with the toxic compound? (ADME):
- Absorbtion
- Distribution
- Metabolism / (de)toxification
- Excretion
è Together this determines what the exposure of the target is to the ultimate toxicant (e.g.
metabolite)
,Metabolism can be seen as a detoxification pathway (metabolites are less toxic than parent
compound), but it can also be the other way around = bioactivation / toxification pathway (in
which the metabolites are more toxic
Threshold of toxicity
- mutagens do not have a threshold of toxicity (B could be mutagenic)
Toxicodynamic factors
- What is the target of this compound? (protein, phospholipid
membrane, mitochondria, DNA, cellular receptor?) & is this aspecific
or highly specific?
Specific: key-and-lock dynamics, antibody-antigens interactions
Aspecific: ROS
- What kind of interaction does the compound undergo with the
target? And what are downstream e]ects?
- ‘So what does the compound do to the body?’
Toxicokinetic factors and toxicodynamic factors (together) can explain:
- Species di]erences in toxicity
- Gender di]erences in toxicity (hormones)
- Organ-selective toxicity (tissue types, permeability, enzymes)
- Interindividual di]erences (genetics, illnesses, predisposition)
- Intraindividual di]erences (within the same person; age)
Brainstorm session
Toxicokinetics in Organ-selective toxicity have to do with the metabolic pathways in that organ
(e.g. presence of certain enzymes that bioactivate), and the function of the organ / tissues the
organ exists of (epithelial cells; perfusion).
Interindividual di]erences in toxicodynamics -> genetic di]erences; Di]erent blood types ->
reactions with antigens; microbiome; Age and disease -> altered metabolic or excretion
capabilities
Intraindividual di]erences (di]erent reactions within the same person, e.g. at a di]erent hour /
moment) -> e.g. pregnant women / di]erential receptor expression across ageing, diet, stress
Biological response: how does the body/cell react to a toxic insult?
- Adaptation (via stress response)
- Toxic response (leading to irreversible cell damage or cell death)
- Similar reactions can be provoked by di]erent types of stress (ischemia, hyperthermia,
oxidative stress, electrophile stress)
,Toxic response or adaptation?
- Is dependent on exposure (concentration and duration) of the toxicant
- Some toxicants reduce ability to respond to stress
Adaptation = ‘harm-induced capability of the organism for increased tolerance of
the harm itself’, by:
- Decreased delivery to the target
- Decreased size/concentration/susceptibility of the target
- Increased capacity for repair (e.g. DNA repair / increased proliferation of cells to replace
damaged cells)
- Compensation of dysfunction
Stress response -> adaptation is often accomplished by stress response reactions, for example:
- Electrophile stress response (nrf-2)
- Heat-shock protein response
- ER-stress response
All result in changes in gene expression
A stress response can also lead to autophagy and apoptosis
Hormesis = sign of adaptation caused by mild forms of stress -> leads to improved
performance e.g. by aquisition of tolerance -> the system now also works better
- E.g. increased DNA repair, anti-oxidant response through more Nrf-2 activity
In case of no adaptation toxic responses can occur, which can be:
- Cell death: necrosis, apoptosis (organ failure)
- Pharmacological / physiological e]ects
- Genotoxicity / mutagenicity
- Carcinogenicity
- Reproduction toxicity, incl. teratogenicity
- Neurotoxicity
- Immunotoxicity, sensitisation
- Irritation (skin, eye)
- Remodelling (fibrosis)
Toxicity vs. adverse drug reactions
Adverse drug reactions (ADR) are toxicity but at pharmaceutical dose levels (bijwerkingen)
(This is toxicity of drugs at normal doses, overdoses lead to intoxications)
- Type A: exaggerated pharmacological e]ect (ON target toxicity)
e.g. if you take two drugs, and the one interveres with the other / polymorphisms (e.g.
expression of CYP enzymes)
- Type B: not related to pharmacological e]ect, not predictable, specific to (some)
individuals (idiosyncreatic drug reactions)
, Some individuals have immune reactions to certain drugs; is very patient specific
- Type C: not related to pharmacological e]ect, often toxic metabolite, predictable (OFF
target toxicity)
e.g. the medicine against morning sickness in pregnancy -> lead to dysmorphia in babies;
probably an interaction with a receptor that is not the target
Adverse outcome pathway = describes etiology of adverse e]ect, from molecular initial event
(MIE) to organism / population response; this assumes a temporal sequence of events
From molecular events on the target to organ e]ects eventually
e.g. drug induced cholestasis = accumulation of bile salts in the liver as they can no longer
enter the bile bladder (look at slides)
- BSEP transports biles salts from the cells into the bile
- if BSEP is inhibited, this leads to bile accumulation in the liver -> inflammation -> apoptosis /
necrosis -> increased enzymes in liver -> cholastasis
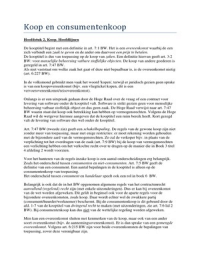
Paracetamol is metabolised (bioactivated) by Cytochrome
p450 -> paracetamol now has a delta+ (in its NAPQI form,
electrophili) that can readily bind to cellular macromolecules,
leading to cell damage and cell death, primarily in the liver
BUT this NAPQI group can be detoxified by GSH (glutathione)
- GSH has a thiol (-SH) group on cysteine, wich is nucleophilic
- This -SH group reacts with the electrophilic NAPQI
Paracetamol can also be metabolized in two di]erent
manners in di]erent organs, which do not produce the ‘toxic’
NAPQI group, and can be excreted through urine
- glucuronidation & sulfation
Because there are su]icient detoxification pathways, paracetamol is safe to use (which means
that under its threshold use, it does not lead to toxicity)
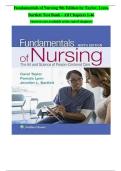
Acrylamide -> it’s metabolite binds to DNA -> leading to liver carcinogenesis in rodents
In humans, the detoxification is more e]icient -> no direct danger
for human health at low concentrations
- glycidamine = toxic metabolite
- can be detoxified by GSH
Summary:
This book was obligatory for this course, and it was used to make this summary:
Boelsterli, U. A. (2007). Mechanistic Toxicology: The Molecular Basis of How Chemicals Disrupt
Biological Targets (2nd ed.). CRC Press. https://doi.org/10.1201/9780367806293
Introduction lecture Chapter 1 & 2
Molecular toxicology and mechanisms of toxicity are required to:
- Estimate risk of human toxicity after exposure to a potentially toxic compound
- Determine toxicity thresholds
- Develop antidotes against acute toxicity
- Development of safe pharmaceuticals
- Develop biomarkers for exposure or toxicity
What is needed for toxicity
- Too high exposure
- Interaction with essential target
- Lack of cell adaptation to the stimulus
Paracelsus’ philosophy: “all compounds are poisons, but it’s the dose that determines if
something is toxic” too much of anything is never good
Dose (+ intrinsic properties) of a compound determine toxicity
- LD50 -> lethal dose (after which an animal is diseased within 50% of exposed animals)
- Potency of a compound has to do with the target it interferes with, and the mechanism
Route of exposure determines toxicity
- Ricin, when administrerd orally, has a di]erent LD50 (need higher dose) then when
injected directly
- Has to do with first pass metabolism and absorption in the intestines
(Internal) exposure determines toxicity -> “all substances are poisons, it is the exposure (of the
target) that determines if a substance is toxic or not”
Toxicokinetic factors; what does the body do with the toxic compound? (ADME):
- Absorbtion
- Distribution
- Metabolism / (de)toxification
- Excretion
è Together this determines what the exposure of the target is to the ultimate toxicant (e.g.
metabolite)
,Metabolism can be seen as a detoxification pathway (metabolites are less toxic than parent
compound), but it can also be the other way around = bioactivation / toxification pathway (in
which the metabolites are more toxic
Threshold of toxicity
- mutagens do not have a threshold of toxicity (B could be mutagenic)
Toxicodynamic factors
- What is the target of this compound? (protein, phospholipid
membrane, mitochondria, DNA, cellular receptor?) & is this aspecific
or highly specific?
Specific: key-and-lock dynamics, antibody-antigens interactions
Aspecific: ROS
- What kind of interaction does the compound undergo with the
target? And what are downstream e]ects?
- ‘So what does the compound do to the body?’
Toxicokinetic factors and toxicodynamic factors (together) can explain:
- Species di]erences in toxicity
- Gender di]erences in toxicity (hormones)
- Organ-selective toxicity (tissue types, permeability, enzymes)
- Interindividual di]erences (genetics, illnesses, predisposition)
- Intraindividual di]erences (within the same person; age)
Brainstorm session
Toxicokinetics in Organ-selective toxicity have to do with the metabolic pathways in that organ
(e.g. presence of certain enzymes that bioactivate), and the function of the organ / tissues the
organ exists of (epithelial cells; perfusion).
Interindividual di]erences in toxicodynamics -> genetic di]erences; Di]erent blood types ->
reactions with antigens; microbiome; Age and disease -> altered metabolic or excretion
capabilities
Intraindividual di]erences (di]erent reactions within the same person, e.g. at a di]erent hour /
moment) -> e.g. pregnant women / di]erential receptor expression across ageing, diet, stress
Biological response: how does the body/cell react to a toxic insult?
- Adaptation (via stress response)
- Toxic response (leading to irreversible cell damage or cell death)
- Similar reactions can be provoked by di]erent types of stress (ischemia, hyperthermia,
oxidative stress, electrophile stress)
,Toxic response or adaptation?
- Is dependent on exposure (concentration and duration) of the toxicant
- Some toxicants reduce ability to respond to stress
Adaptation = ‘harm-induced capability of the organism for increased tolerance of
the harm itself’, by:
- Decreased delivery to the target
- Decreased size/concentration/susceptibility of the target
- Increased capacity for repair (e.g. DNA repair / increased proliferation of cells to replace
damaged cells)
- Compensation of dysfunction
Stress response -> adaptation is often accomplished by stress response reactions, for example:
- Electrophile stress response (nrf-2)
- Heat-shock protein response
- ER-stress response
All result in changes in gene expression
A stress response can also lead to autophagy and apoptosis
Hormesis = sign of adaptation caused by mild forms of stress -> leads to improved
performance e.g. by aquisition of tolerance -> the system now also works better
- E.g. increased DNA repair, anti-oxidant response through more Nrf-2 activity
In case of no adaptation toxic responses can occur, which can be:
- Cell death: necrosis, apoptosis (organ failure)
- Pharmacological / physiological e]ects
- Genotoxicity / mutagenicity
- Carcinogenicity
- Reproduction toxicity, incl. teratogenicity
- Neurotoxicity
- Immunotoxicity, sensitisation
- Irritation (skin, eye)
- Remodelling (fibrosis)
Toxicity vs. adverse drug reactions
Adverse drug reactions (ADR) are toxicity but at pharmaceutical dose levels (bijwerkingen)
(This is toxicity of drugs at normal doses, overdoses lead to intoxications)
- Type A: exaggerated pharmacological e]ect (ON target toxicity)
e.g. if you take two drugs, and the one interveres with the other / polymorphisms (e.g.
expression of CYP enzymes)
- Type B: not related to pharmacological e]ect, not predictable, specific to (some)
individuals (idiosyncreatic drug reactions)
, Some individuals have immune reactions to certain drugs; is very patient specific
- Type C: not related to pharmacological e]ect, often toxic metabolite, predictable (OFF
target toxicity)
e.g. the medicine against morning sickness in pregnancy -> lead to dysmorphia in babies;
probably an interaction with a receptor that is not the target
Adverse outcome pathway = describes etiology of adverse e]ect, from molecular initial event
(MIE) to organism / population response; this assumes a temporal sequence of events
From molecular events on the target to organ e]ects eventually
e.g. drug induced cholestasis = accumulation of bile salts in the liver as they can no longer
enter the bile bladder (look at slides)
- BSEP transports biles salts from the cells into the bile
- if BSEP is inhibited, this leads to bile accumulation in the liver -> inflammation -> apoptosis /
necrosis -> increased enzymes in liver -> cholastasis
Paracetamol is metabolised (bioactivated) by Cytochrome
p450 -> paracetamol now has a delta+ (in its NAPQI form,
electrophili) that can readily bind to cellular macromolecules,
leading to cell damage and cell death, primarily in the liver
BUT this NAPQI group can be detoxified by GSH (glutathione)
- GSH has a thiol (-SH) group on cysteine, wich is nucleophilic
- This -SH group reacts with the electrophilic NAPQI
Paracetamol can also be metabolized in two di]erent
manners in di]erent organs, which do not produce the ‘toxic’
NAPQI group, and can be excreted through urine
- glucuronidation & sulfation
Because there are su]icient detoxification pathways, paracetamol is safe to use (which means
that under its threshold use, it does not lead to toxicity)
Acrylamide -> it’s metabolite binds to DNA -> leading to liver carcinogenesis in rodents
In humans, the detoxification is more e]icient -> no direct danger
for human health at low concentrations
- glycidamine = toxic metabolite
- can be detoxified by GSH
Summary: