CONDITION :
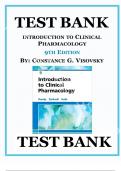
Hypertension
PATHOPHYSIOLOGY : RISK FACTORS :
Plaquebuild u Age
*
* Vascular
changes progresses Narrow lumen
-
Exacubation
a Gender Men have BP up 65
higher
* - to
↑ Total Peripheral resistance Arterial BP
*
Sympathetic Nervous Leads to vasoconstriction - =
system activity
increases >
Black Africant Black Carribbean
Ethnicity
-
* - are more at risk .
& cause of
Antigensen
release renin - Il production
Genetics
-Adrenal
* gland o n s e
Act on SA node - HR = ↑CO - ↑BP
ComorbiditieSepapa
*
Ventricular
myocardium - 4 Contractility - NSV + CO - 4 BP
issue
DecreasedSaltexcretio
* Natretention Blood volume -,
Lifesty, a
*
- vasoconstrictor -
> ↓ Total peripheral resistance
a l t intake
Anxiety
*
+ Stress
*
Medicationde
RED FLAGS AND COMPLICATIONS : SIGNS : SYMPTOMS :
D F L AG S
Stage 1 :
GMHg(CLINICAL * Headaches
Eye Vessel
haemorrhage
135/85mmHg (ABPM)
< -
RetinopathyBlurred i
* a
3
* Headaches
2
* Visual disturbances Stage : > 160/100 (CLINICAL
* Naused
Malignant HTN- TREMEDIATELY 7150/95 (ABPM)
Dizziness
+ Emenis *
* Chest pain
Stage 3 : >180/110 (CLINICAL
*
Dyspnea
TYPES * Nausea +
vomiting
fail
MATOMScaentica
* Heart
1 HTN : No k n ow n
Develops
gradually 3
cause
presentation
-
- > 404TPR
401CO
*
*
Confusion
Anxiety
#MyardInadsuppata crosis 2 HTN
:Caused by combobidysersaa
*
*
Arrhythmia
Buzzing in ears
* Retinopathy >
-
Due to we a ke n e d vessel wa l l
nephrosclerosisP ↳ Antidepressantraceptives
Renal
Usually 40.
failure + <
* AK1
>
* Nose bleeds
Accelerated
*
Aneursym HTN : Show
signs of retinal
damage
Malignant HTN
↑ Risk of Cardiovascular event .
I
VESTIGATION : TREATMENT :
THARMACOLOGICAL
#FEST YLE
ADVICE
# Measure
-
Clinical + ABPM blood pressure -
>
140/90mmHg = HTN
STEP 1 : UNDER55
-> Consider * Exercise
White Coat HTN
* ACE (Lisinopril , STEP2 Add CCB
.
Inhibitor Ramipril) .
↳ * Reduce alcohol
UrinanalysisHaematura kidney
* Causes vasoconstriction
disa ns
ST * Diet
ARBs CostaCaduartan
*
* Test for diabetes >
-
Hb1AC * Reduce salts
OVER 55
* Test for GFR + Urine Albumin -
Sign of CKD
* Calcium Channel Blockers (Amlodipine) STEPAdd
* Stop smoking
ACEO , ARB
Examine
* fundi -
Retinopathy ↳ Alsoused
for Black African or Carribean
origin
* ECG
* Thiazide-like Diuretic (Indapamide
* Assess cardiovascular
riskhaday came
↳ If CCB doesn't wo r k
STEP 3 :
Optimise Step 2 first
Combine (CB ARB/ACE and diuretic
,
STEP4 : K"SPARING DIURETIC
↳ Spironolactone Bendrofluremthiazide
,
ALPHABLOCKE parazosin
,
Terazosin
BETA BLOCKER
↳ Atenelol
, Bisoprolo
, CONDITION: : Acute
Coronary Syndrome
PATHOPHYSIOLOGY :
PATHOPHYSOGo
RISKFACTOR
RISK FACTORS :
S
Gender
S
* >
-
Male = ↑ Risk
*
Age
- Embolism *
Family History Non-modifiable
Ethnicity
to Cardiac muscle *
Leads
HIGH O2 DEMAND -
Hyper consumption of O2 - ACUTEMYOCARDIAL INFARCTION
death
&tanycardia
2
. Highmotaiyaa
are
S
Gender
affirming medications
*
ony
= Thicker
Myocardium ~ 40 minute
Smoking
*
Exercise/exertion of occlusion
*
Hypertension
*
Pre-existing plaques can cause
disruption * Diabetes
Modifiable
ruptedesc
*
Hyperlipademia
CONSEQUENCES is
*
High Choletrol
Impaired pump action ↑ load-ESV ++ SVV
*
Obesity
*
Myocardium
>
-
Due Effect of
*
Sedentary Life
*
Myocardium stiffening -> to
scarring
- ATP on
actin-myosin -
Impaired diastolic filling
*
Pulmonary Congestion +
dyspnea Back How Cardiac failure Causes
hypertrophy
-
+ >
-
* Abnormal ventricular contraction >
-
Lactic acid produced - Low ATP - Can lead to acidosis + infarction
RED FLAGS AND COMPLICATIONS :
REDFLAGS SIGNS : SYMPTOMS :
States
Myocardial Ischaemic
RE D
FLAGS
Unstable
~ * Chest pain - Relieved - Stable
angina
* Pain radiates
Angina ↳ Sustained-Unstable
that 15 minutes NSTEMI STEMI
angina
-
>
↳ ↳ cheet pain 'elephant on chent'
CHARACTERDuring
MI
Heavy
occlusion
-
occuymna
vom
Unstable blockage partial Full
↳ RADIATION - Left side
* Radiation
of pain - Left sided >
-
Can travel to shoulders + neck
> shoulder ↑ Risk of STEMI ↑ Risk of Cardia (
death Elevated UR
-
*
>
-
Neck + Jaw
Stinterval
Breathlessness *
Indigestion
Intervaldepressin
* +
Sweating + Nausea and e m e r i St a
elevation
↑ Risk
Dyspnea
of M1 *
*
Systolic pressure
90mmHg
Swearing
*
* Abrupt deterioration of
angina
*
Hypotension
COMPLICATIONS * Fatiuge
* Thrombosis
* Death * Nausea + Emesis
* Heart Failure
Sinustachycardia bradycara
*
Aneursym
*
Myocardial Rupture
* Pericarditis
VESTIGATION TREATME
TREATMENT
N-i:
range
ON : INITAL
Mor phine (tantiemetic
Oxygen (194 %
Nitrate
a
Aspirin (300mg)
of Q
- Development
> STEMI NSTEMI
* ECG - ST interval + T wave
Aspirin 300 +
Fondaparinux OR
MEDICAL REPERFUSION Unfractionated Heparin
* Assess pain characteristics Radiation n
GRACEscore
>
- Character
Angiography + PCI
,
great Low Risk < 3%
Bleeding Misk High Risk > 3%
* Blood tests Troponin T Troponin more cardio
specific Anti-coag
patient
>
- + 1 >
-
I
↳ Ticagremm
- YES
> Serum level ↑ With 3-12 his of pain
a
Aspirin paint
Biomarkers -
Fatty acid
binding protein
Clopigrel +
Clopidgrel Parasugeas -c
+ Aspirin
Btype
>
Passea
natriuretic peptide
-
>
-
Ischaemia
modified albumin P TO M R ECANGINA)
LIEF Clopidge Klopig
GTN If second dose doesn't
workafterI
Co-peptic * minutea
Spray
>
-
-
* CCB or Beta-blocker - I F INTOLERANT--NICORANDIL
Echo
*
diagram
-> Shows loss
of myocardium -> NITRATE
Y RANOLAZINE
SECON DA RY
PREVENTION
Statin -> Lower Cholestrol = Reduce risk (Atrovastatin)
ACE
inhibtor-ManageHTN risk
Anti-platelets (dual)
Beta blockers
+ PPI to counter antiplatelet
+ GTN
, CONDITION : Heart Failure
PATHOPHYSIOLOGY : RISK FACTORS :
M A S DYSFUNCTION
TO L I C
*
* LV Causes stiffer muscle -t Arterial pressure
Obesity
Hypertrophy
->
*
Angina M1+ Reduces ATP-
-
> ↓
Actin-myosin contraction
*
High Cholestro
OBSTRUCTION OF
*
Hypertension
S
LV FILLING
StDSTO
-
* Diabetes
* Cardiac tamponade
↑ e i a l pressure
* Narrowed mitral value Smoking
*
IMPAIRED CONTRACTILITY
*
Sedentary Lifestyle
*
Congenital h e ar t disease
-
Myocardial Death of Cardiac muscle
3
* infarction >
LV
systolic dysfunction Coronary Heart Diseone
-
*
* Overstretched values Le a k-f Force contraction
>
f
Arrhythmia
-
*
O M P RCARDIAC
OMI FUNCTION
SED
*
History of M
huncion ofVaricodation volume
SV and (0 ↓ Pressure
*
med - >
-
Triggers Sympathetic Om demand
↳ ↓V
filling
-
Pulmonary Congestion -
Due to t pressure
REDFLAGS AND COMPLICATIONS : SIGNS : SYMPTOMS :
* Pink White
CLASSIFICATIONS Or
foamy sputum
SRED
FLASiness * Oedema-Ankles +
Legs
CLASSI : No
>
symptoms during activity
.
-
*
CLASS11 Dyspnea
Dyspnea Triggered by physical activity
:
> atrest
* Cold perphries
- .
Angina : Triggeredbymina'activia
,
>
-
at rest
at rest.
*
Hypotension
Hypokalemia
>
-
Reduced
ALPRESENTATION How-Antiogensen-renin system
* Urine cames fluid retention .
Confusion and
dehydration 40 %
>
-
-
* Raised JVP
Unable to m ove without p a n * Atrial Fibrillation
-
Backlog of pressure in vessel
↓ CO Consolidation
>
Lung
-
*
>
-
COMPLETION Compensatory High
* Heart Rate - > GOBPM
*
* Depression
*
High NT-proBNP->Age dependent >
-
< 75
years
: 1125
Fatiugeend Liver
- 7 5 years Lack of appetite
>
2450
-
:
*
Anaeuia idney Disease
* Loss of
weight
*
Change in sleep >
Paraxysmal nocturnal
dyspnea
-
* Acute
Kidney Injury
* Sudden Cardiac death
* Can't sleep Hat
Lying
VESTIGATION : TREATMENT :
* Measure NT-proBNP # Loop diuretic (Furesomide
Congestive symptome
to
manage
ECG
*
Arrange
* Chest
X-tray #DEF
ComborditeTwic
-HDTAC *
* Blood
testeeG Manage heartd e e
* Assess what
underlying cames
F r E F (FIVE PILLARS OF TREATMENT
#
* Natriuretic peptide levels
* Determine if it is HFrEForHFpEF- Assess ejection Fraction Echo
diagram
> -
Arboasdine
3
ACEi or
est line
Beta Blocker -> With ACEi
-
Use
-> cardio
specific
>
Monitor fluid retention
-
spiranalactone
diuretic
MRAottacium Spaing na se
3
SGLT2i - Must include indication
E Ivabradine - Reduce #R
Dipagaflozin to
-
g 3rd
.
Line -- In addition
So
-
A R N i Sacubril/Valsartan Digoxin- Anti-arrhythmic
Hypertension
PATHOPHYSIOLOGY : RISK FACTORS :
Plaquebuild u Age
*
* Vascular
changes progresses Narrow lumen
-
Exacubation
a Gender Men have BP up 65
higher
* - to
↑ Total Peripheral resistance Arterial BP
*
Sympathetic Nervous Leads to vasoconstriction - =
system activity
increases >
Black Africant Black Carribbean
Ethnicity
-
* - are more at risk .
& cause of
Antigensen
release renin - Il production
Genetics
-Adrenal
* gland o n s e
Act on SA node - HR = ↑CO - ↑BP
ComorbiditieSepapa
*
Ventricular
myocardium - 4 Contractility - NSV + CO - 4 BP
issue
DecreasedSaltexcretio
* Natretention Blood volume -,
Lifesty, a
*
- vasoconstrictor -
> ↓ Total peripheral resistance
a l t intake
Anxiety
*
+ Stress
*
Medicationde
RED FLAGS AND COMPLICATIONS : SIGNS : SYMPTOMS :
D F L AG S
Stage 1 :
GMHg(CLINICAL * Headaches
Eye Vessel
haemorrhage
135/85mmHg (ABPM)
< -
RetinopathyBlurred i
* a
3
* Headaches
2
* Visual disturbances Stage : > 160/100 (CLINICAL
* Naused
Malignant HTN- TREMEDIATELY 7150/95 (ABPM)
Dizziness
+ Emenis *
* Chest pain
Stage 3 : >180/110 (CLINICAL
*
Dyspnea
TYPES * Nausea +
vomiting
fail
MATOMScaentica
* Heart
1 HTN : No k n ow n
Develops
gradually 3
cause
presentation
-
- > 404TPR
401CO
*
*
Confusion
Anxiety
#MyardInadsuppata crosis 2 HTN
:Caused by combobidysersaa
*
*
Arrhythmia
Buzzing in ears
* Retinopathy >
-
Due to we a ke n e d vessel wa l l
nephrosclerosisP ↳ Antidepressantraceptives
Renal
Usually 40.
failure + <
* AK1
>
* Nose bleeds
Accelerated
*
Aneursym HTN : Show
signs of retinal
damage
Malignant HTN
↑ Risk of Cardiovascular event .
I
VESTIGATION : TREATMENT :
THARMACOLOGICAL
#FEST YLE
ADVICE
# Measure
-
Clinical + ABPM blood pressure -
>
140/90mmHg = HTN
STEP 1 : UNDER55
-> Consider * Exercise
White Coat HTN
* ACE (Lisinopril , STEP2 Add CCB
.
Inhibitor Ramipril) .
↳ * Reduce alcohol
UrinanalysisHaematura kidney
* Causes vasoconstriction
disa ns
ST * Diet
ARBs CostaCaduartan
*
* Test for diabetes >
-
Hb1AC * Reduce salts
OVER 55
* Test for GFR + Urine Albumin -
Sign of CKD
* Calcium Channel Blockers (Amlodipine) STEPAdd
* Stop smoking
ACEO , ARB
Examine
* fundi -
Retinopathy ↳ Alsoused
for Black African or Carribean
origin
* ECG
* Thiazide-like Diuretic (Indapamide
* Assess cardiovascular
riskhaday came
↳ If CCB doesn't wo r k
STEP 3 :
Optimise Step 2 first
Combine (CB ARB/ACE and diuretic
,
STEP4 : K"SPARING DIURETIC
↳ Spironolactone Bendrofluremthiazide
,
ALPHABLOCKE parazosin
,
Terazosin
BETA BLOCKER
↳ Atenelol
, Bisoprolo
, CONDITION: : Acute
Coronary Syndrome
PATHOPHYSIOLOGY :
PATHOPHYSOGo
RISKFACTOR
RISK FACTORS :
S
Gender
S
* >
-
Male = ↑ Risk
*
Age
- Embolism *
Family History Non-modifiable
Ethnicity
to Cardiac muscle *
Leads
HIGH O2 DEMAND -
Hyper consumption of O2 - ACUTEMYOCARDIAL INFARCTION
death
&tanycardia
2
. Highmotaiyaa
are
S
Gender
affirming medications
*
ony
= Thicker
Myocardium ~ 40 minute
Smoking
*
Exercise/exertion of occlusion
*
Hypertension
*
Pre-existing plaques can cause
disruption * Diabetes
Modifiable
ruptedesc
*
Hyperlipademia
CONSEQUENCES is
*
High Choletrol
Impaired pump action ↑ load-ESV ++ SVV
*
Obesity
*
Myocardium
>
-
Due Effect of
*
Sedentary Life
*
Myocardium stiffening -> to
scarring
- ATP on
actin-myosin -
Impaired diastolic filling
*
Pulmonary Congestion +
dyspnea Back How Cardiac failure Causes
hypertrophy
-
+ >
-
* Abnormal ventricular contraction >
-
Lactic acid produced - Low ATP - Can lead to acidosis + infarction
RED FLAGS AND COMPLICATIONS :
REDFLAGS SIGNS : SYMPTOMS :
States
Myocardial Ischaemic
RE D
FLAGS
Unstable
~ * Chest pain - Relieved - Stable
angina
* Pain radiates
Angina ↳ Sustained-Unstable
that 15 minutes NSTEMI STEMI
angina
-
>
↳ ↳ cheet pain 'elephant on chent'
CHARACTERDuring
MI
Heavy
occlusion
-
occuymna
vom
Unstable blockage partial Full
↳ RADIATION - Left side
* Radiation
of pain - Left sided >
-
Can travel to shoulders + neck
> shoulder ↑ Risk of STEMI ↑ Risk of Cardia (
death Elevated UR
-
*
>
-
Neck + Jaw
Stinterval
Breathlessness *
Indigestion
Intervaldepressin
* +
Sweating + Nausea and e m e r i St a
elevation
↑ Risk
Dyspnea
of M1 *
*
Systolic pressure
90mmHg
Swearing
*
* Abrupt deterioration of
angina
*
Hypotension
COMPLICATIONS * Fatiuge
* Thrombosis
* Death * Nausea + Emesis
* Heart Failure
Sinustachycardia bradycara
*
Aneursym
*
Myocardial Rupture
* Pericarditis
VESTIGATION TREATME
TREATMENT
N-i:
range
ON : INITAL
Mor phine (tantiemetic
Oxygen (194 %
Nitrate
a
Aspirin (300mg)
of Q
- Development
> STEMI NSTEMI
* ECG - ST interval + T wave
Aspirin 300 +
Fondaparinux OR
MEDICAL REPERFUSION Unfractionated Heparin
* Assess pain characteristics Radiation n
GRACEscore
>
- Character
Angiography + PCI
,
great Low Risk < 3%
Bleeding Misk High Risk > 3%
* Blood tests Troponin T Troponin more cardio
specific Anti-coag
patient
>
- + 1 >
-
I
↳ Ticagremm
- YES
> Serum level ↑ With 3-12 his of pain
a
Aspirin paint
Biomarkers -
Fatty acid
binding protein
Clopigrel +
Clopidgrel Parasugeas -c
+ Aspirin
Btype
>
Passea
natriuretic peptide
-
>
-
Ischaemia
modified albumin P TO M R ECANGINA)
LIEF Clopidge Klopig
GTN If second dose doesn't
workafterI
Co-peptic * minutea
Spray
>
-
-
* CCB or Beta-blocker - I F INTOLERANT--NICORANDIL
Echo
*
diagram
-> Shows loss
of myocardium -> NITRATE
Y RANOLAZINE
SECON DA RY
PREVENTION
Statin -> Lower Cholestrol = Reduce risk (Atrovastatin)
ACE
inhibtor-ManageHTN risk
Anti-platelets (dual)
Beta blockers
+ PPI to counter antiplatelet
+ GTN
, CONDITION : Heart Failure
PATHOPHYSIOLOGY : RISK FACTORS :
M A S DYSFUNCTION
TO L I C
*
* LV Causes stiffer muscle -t Arterial pressure
Obesity
Hypertrophy
->
*
Angina M1+ Reduces ATP-
-
> ↓
Actin-myosin contraction
*
High Cholestro
OBSTRUCTION OF
*
Hypertension
S
LV FILLING
StDSTO
-
* Diabetes
* Cardiac tamponade
↑ e i a l pressure
* Narrowed mitral value Smoking
*
IMPAIRED CONTRACTILITY
*
Sedentary Lifestyle
*
Congenital h e ar t disease
-
Myocardial Death of Cardiac muscle
3
* infarction >
LV
systolic dysfunction Coronary Heart Diseone
-
*
* Overstretched values Le a k-f Force contraction
>
f
Arrhythmia
-
*
O M P RCARDIAC
OMI FUNCTION
SED
*
History of M
huncion ofVaricodation volume
SV and (0 ↓ Pressure
*
med - >
-
Triggers Sympathetic Om demand
↳ ↓V
filling
-
Pulmonary Congestion -
Due to t pressure
REDFLAGS AND COMPLICATIONS : SIGNS : SYMPTOMS :
* Pink White
CLASSIFICATIONS Or
foamy sputum
SRED
FLASiness * Oedema-Ankles +
Legs
CLASSI : No
>
symptoms during activity
.
-
*
CLASS11 Dyspnea
Dyspnea Triggered by physical activity
:
> atrest
* Cold perphries
- .
Angina : Triggeredbymina'activia
,
>
-
at rest
at rest.
*
Hypotension
Hypokalemia
>
-
Reduced
ALPRESENTATION How-Antiogensen-renin system
* Urine cames fluid retention .
Confusion and
dehydration 40 %
>
-
-
* Raised JVP
Unable to m ove without p a n * Atrial Fibrillation
-
Backlog of pressure in vessel
↓ CO Consolidation
>
Lung
-
*
>
-
COMPLETION Compensatory High
* Heart Rate - > GOBPM
*
* Depression
*
High NT-proBNP->Age dependent >
-
< 75
years
: 1125
Fatiugeend Liver
- 7 5 years Lack of appetite
>
2450
-
:
*
Anaeuia idney Disease
* Loss of
weight
*
Change in sleep >
Paraxysmal nocturnal
dyspnea
-
* Acute
Kidney Injury
* Sudden Cardiac death
* Can't sleep Hat
Lying
VESTIGATION : TREATMENT :
* Measure NT-proBNP # Loop diuretic (Furesomide
Congestive symptome
to
manage
ECG
*
Arrange
* Chest
X-tray #DEF
ComborditeTwic
-HDTAC *
* Blood
testeeG Manage heartd e e
* Assess what
underlying cames
F r E F (FIVE PILLARS OF TREATMENT
#
* Natriuretic peptide levels
* Determine if it is HFrEForHFpEF- Assess ejection Fraction Echo
diagram
> -
Arboasdine
3
ACEi or
est line
Beta Blocker -> With ACEi
-
Use
-> cardio
specific
>
Monitor fluid retention
-
spiranalactone
diuretic
MRAottacium Spaing na se
3
SGLT2i - Must include indication
E Ivabradine - Reduce #R
Dipagaflozin to
-
g 3rd
.
Line -- In addition
So
-
A R N i Sacubril/Valsartan Digoxin- Anti-arrhythmic