Mental health
Anxiety disorders
Michael Kyrios
Richard Moulding
Assessment and management in
Maja Nedeljkovic
general practice
Anxiety is a normal human physiological mechanism
Background
designed to help the body respond to a threat. The
Anxiety is a normal physiological response to a threat.
autonomic changes that occur in anxiety are essential to
Anxiety disorders occur when this normal physiological
response is associated with high levels of autonomic avoid danger and moderate anxiety can actually improve
arousal, erroneous cognitions and dysfunctional coping performance. However, when anxiety is associated
strategies. Anxiety disorders are highly prevalent and with very high levels of autonomic arousal, erroneous
present commonly to general practice. Anxiety disorders cognitions including exaggerated threat perceptions
are often comorbid with other psychiatric and medical and dysfunctional coping strategies, it can result in
disorders and may be associated with significant morbidity. significant distress and impairment in work, school,
Objective family, relationships, and/or activities of daily living.
This article describes the diagnosis, assessment and Patients presenting with anxiety symptoms in the general
management of anxiety disorders in the general practice practice setting do not always fit the criteria for a specific
setting. anxiety disorder. However, it is important for the general
practitioner to know how to assess patients for specific
Discussion
anxiety disorders and the basic principles of management
Assessment in patients presenting with anxiety symptoms
involves excluding a medical cause, identifying features of these disorders. Equally, GPs need strategies to manage
of specific anxiety disorders as well as other coexisting patients with distressing anxiety symptoms who do not
psychiatric disorders, and assessing the degree of fulfil the criteria for the diagnosis of a specific anxiety
distress. Management options include psychoeducation, disorder and/or where the anxiety coexists with another
psychological treatments (particularly cognitive behaviour mental health disorder (such as depression), substance
therapy) and pharmacological treatments. Patients with abuse or medical condition.1
a diagnosis of an anxiety disorder can access Medicare
funded psychological care under a number of Australian Twelve month prevalence rates in Australia indicate that anxiety
government initiatives. Selective serotonin reuptake disorders are the most common mental health problem, affecting
inhibitors and serotonin norepinephrine reuptake inhibitors
14.4% of the population (although some people experienced more
are the first line pharmacological agents used to treat
than one type of anxiety disorder). Post-traumatic stress disorder
anxiety disorders. Regular review is vital to monitor for
(PTSD) is the most widespread affecting 6.4% of the population,
clinical improvement and more complex presentations may
require specialist psychological or psychiatric referral. followed by social phobia (4.7%), agoraphobia (2.8%), generalised
anxiety disorder (GAD, 2.7%), panic disorder (2.6%), and obsessive
Keywords: anxiety disorders; mental health; treatment compulsive disorder (OCD, 1.9%).2 Women experienced higher rates
than men (18% and 11% respectively), and the highest rate of anxiety
disorders was in the 35–44 years age group (18%). One in 5 women
and one in 10 men report a specific phobia.3 General practice is often
the first port-of-call for patients with anxiety disorders; one in 10
people experiencing an anxiety disorder within the past 12 months
visited a GP for their mental health problems but did not receive care
from any other provider.4 The Bettering the Evaluation and Care of
Health program showed that GPs treat psychological problems at a
370 Reprinted from Australian Family Physician Vol. 40, No. 6, JUNE 2011
, rate of 11.5 per 100 encounters and anxiety is the second commonest disorder such as depression, bipolar disorder or a psychotic disorder.
psychological problem managed after depression.5 It is important to screen for these diagnoses at the initial assessment.
For example, the ruminative thoughts seen in depression can be similar
Assessment to worry, but they usually are more concerned with past events, self
Initial assessment should begin with a focused history. Allow criticism and guilt, rather than future events. If a specific anxiety
the patient to describe the symptoms they find most concerning disorder is diagnosed, there is a high risk that the patient will also have
and enquire about substance use as well as symptoms that may a psychiatric comorbidity or significant substance use. For example, the
be suggestive of a medical condition. Physical examination and presence of GAD increases the likelihood of having depression by an
investigations should concentrate on excluding an underlying medical odds ratio of 28.9.7 Anxiety disorders themselves tend to co-occur and
cause. Medical conditions that can be associated with anxiety include:6 the greater the comorbidity, the greater the likelihood of help seeking.8
• hypoglycaemia Hypochondriasis is another important diagnosis to consider in the
• hyper- or hypo-thyroidism
• cardiac disorders
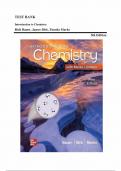
• chronic respiratory disease Exaggerated autonomic Does the patient have
• vitamin B deficiency arousal as a reaction to a medical condition or No
perceived danger/s substance related problem?
• inner ear conditions
• acute reactions to aspartame
Are there possible
• withdrawal from benzodiazepines.
Yes co-occurring anxiety Yes
If there is no evidence of a medical cause problems?
for the patient’s symptoms, assessment
should move on to looking for features
What signs or symptoms does the
of specific anxiety disorders as well as patient report?
other coexisting psychiatric disorders,
and assessing the degree of distress. Specific triggers causing anxiety and
Consider simple phobia
avoidance
Symptoms of specific
anxiety disorders
Recurrent panic attacks, catastrophising
Consider panic disorder
Diagnosis of specific anxiety disorders about anxiety and panic symptoms
involves identification of a specific focus
for the anxiety. For instance, if a patient Avoidance of open or crowded spaces with
Consider agoraphobia
has panic attacks and catastrophises accompanying worry about panic
about these as indicating an imminent
heart attack/suffocation, a diagnosis Chronic, exaggerated, excessive,
of panic disorder may be warranted. unwarranted worries and preoccupation Consider generalised
However, if anxiety or the panic attacks about future or everyday issues with anxiety disorder
occur only on exposure to social associated tension
situations, then social phobia may be
the diagnosis (Figure 1). Full diagnostic Excessive preoccupation about perceived
criteria are available in the Diagnostic criticisms or being judged negatively Consider social phobia
by others with associated social avoidance
and Statistical Manual of Mental
or anxiety
Disorders (4th edn, text revision) (DSM-
IV-TR).6 Of course, in the general practice
Preoccupation and recurrent
setting, many patients do not fit neatly Consider post-traumatic
re-experiencing of traumatic event/s,
into this framework and have symptoms stress disorder
persistent hyperarousal and avoidance
of multiple disorders without fulfilling the
criteria for a specific disorder. Unwanted intrusive recurrent thoughts,
images or urges leading to distress or Consider obsessive
Coexisting psychiatric discomfort and/or excessive, ritualised compulsive disorder
disorders compulsive responses
Anxiety may be a symptom of, or coexist
Figure 1. Differential diagnosis of anxiety disorders
with, another underlying psychiatric
Reprinted from Australian Family Physician Vol. 40, No. 6, JUNE 2011 371
Anxiety disorders
Michael Kyrios
Richard Moulding
Assessment and management in
Maja Nedeljkovic
general practice
Anxiety is a normal human physiological mechanism
Background
designed to help the body respond to a threat. The
Anxiety is a normal physiological response to a threat.
autonomic changes that occur in anxiety are essential to
Anxiety disorders occur when this normal physiological
response is associated with high levels of autonomic avoid danger and moderate anxiety can actually improve
arousal, erroneous cognitions and dysfunctional coping performance. However, when anxiety is associated
strategies. Anxiety disorders are highly prevalent and with very high levels of autonomic arousal, erroneous
present commonly to general practice. Anxiety disorders cognitions including exaggerated threat perceptions
are often comorbid with other psychiatric and medical and dysfunctional coping strategies, it can result in
disorders and may be associated with significant morbidity. significant distress and impairment in work, school,
Objective family, relationships, and/or activities of daily living.
This article describes the diagnosis, assessment and Patients presenting with anxiety symptoms in the general
management of anxiety disorders in the general practice practice setting do not always fit the criteria for a specific
setting. anxiety disorder. However, it is important for the general
practitioner to know how to assess patients for specific
Discussion
anxiety disorders and the basic principles of management
Assessment in patients presenting with anxiety symptoms
involves excluding a medical cause, identifying features of these disorders. Equally, GPs need strategies to manage
of specific anxiety disorders as well as other coexisting patients with distressing anxiety symptoms who do not
psychiatric disorders, and assessing the degree of fulfil the criteria for the diagnosis of a specific anxiety
distress. Management options include psychoeducation, disorder and/or where the anxiety coexists with another
psychological treatments (particularly cognitive behaviour mental health disorder (such as depression), substance
therapy) and pharmacological treatments. Patients with abuse or medical condition.1
a diagnosis of an anxiety disorder can access Medicare
funded psychological care under a number of Australian Twelve month prevalence rates in Australia indicate that anxiety
government initiatives. Selective serotonin reuptake disorders are the most common mental health problem, affecting
inhibitors and serotonin norepinephrine reuptake inhibitors
14.4% of the population (although some people experienced more
are the first line pharmacological agents used to treat
than one type of anxiety disorder). Post-traumatic stress disorder
anxiety disorders. Regular review is vital to monitor for
(PTSD) is the most widespread affecting 6.4% of the population,
clinical improvement and more complex presentations may
require specialist psychological or psychiatric referral. followed by social phobia (4.7%), agoraphobia (2.8%), generalised
anxiety disorder (GAD, 2.7%), panic disorder (2.6%), and obsessive
Keywords: anxiety disorders; mental health; treatment compulsive disorder (OCD, 1.9%).2 Women experienced higher rates
than men (18% and 11% respectively), and the highest rate of anxiety
disorders was in the 35–44 years age group (18%). One in 5 women
and one in 10 men report a specific phobia.3 General practice is often
the first port-of-call for patients with anxiety disorders; one in 10
people experiencing an anxiety disorder within the past 12 months
visited a GP for their mental health problems but did not receive care
from any other provider.4 The Bettering the Evaluation and Care of
Health program showed that GPs treat psychological problems at a
370 Reprinted from Australian Family Physician Vol. 40, No. 6, JUNE 2011
, rate of 11.5 per 100 encounters and anxiety is the second commonest disorder such as depression, bipolar disorder or a psychotic disorder.
psychological problem managed after depression.5 It is important to screen for these diagnoses at the initial assessment.
For example, the ruminative thoughts seen in depression can be similar
Assessment to worry, but they usually are more concerned with past events, self
Initial assessment should begin with a focused history. Allow criticism and guilt, rather than future events. If a specific anxiety
the patient to describe the symptoms they find most concerning disorder is diagnosed, there is a high risk that the patient will also have
and enquire about substance use as well as symptoms that may a psychiatric comorbidity or significant substance use. For example, the
be suggestive of a medical condition. Physical examination and presence of GAD increases the likelihood of having depression by an
investigations should concentrate on excluding an underlying medical odds ratio of 28.9.7 Anxiety disorders themselves tend to co-occur and
cause. Medical conditions that can be associated with anxiety include:6 the greater the comorbidity, the greater the likelihood of help seeking.8
• hypoglycaemia Hypochondriasis is another important diagnosis to consider in the
• hyper- or hypo-thyroidism
• cardiac disorders
• chronic respiratory disease Exaggerated autonomic Does the patient have
• vitamin B deficiency arousal as a reaction to a medical condition or No
perceived danger/s substance related problem?
• inner ear conditions
• acute reactions to aspartame
Are there possible
• withdrawal from benzodiazepines.
Yes co-occurring anxiety Yes
If there is no evidence of a medical cause problems?
for the patient’s symptoms, assessment
should move on to looking for features
What signs or symptoms does the
of specific anxiety disorders as well as patient report?
other coexisting psychiatric disorders,
and assessing the degree of distress. Specific triggers causing anxiety and
Consider simple phobia
avoidance
Symptoms of specific
anxiety disorders
Recurrent panic attacks, catastrophising
Consider panic disorder
Diagnosis of specific anxiety disorders about anxiety and panic symptoms
involves identification of a specific focus
for the anxiety. For instance, if a patient Avoidance of open or crowded spaces with
Consider agoraphobia
has panic attacks and catastrophises accompanying worry about panic
about these as indicating an imminent
heart attack/suffocation, a diagnosis Chronic, exaggerated, excessive,
of panic disorder may be warranted. unwarranted worries and preoccupation Consider generalised
However, if anxiety or the panic attacks about future or everyday issues with anxiety disorder
occur only on exposure to social associated tension
situations, then social phobia may be
the diagnosis (Figure 1). Full diagnostic Excessive preoccupation about perceived
criteria are available in the Diagnostic criticisms or being judged negatively Consider social phobia
by others with associated social avoidance
and Statistical Manual of Mental
or anxiety
Disorders (4th edn, text revision) (DSM-
IV-TR).6 Of course, in the general practice
Preoccupation and recurrent
setting, many patients do not fit neatly Consider post-traumatic
re-experiencing of traumatic event/s,
into this framework and have symptoms stress disorder
persistent hyperarousal and avoidance
of multiple disorders without fulfilling the
criteria for a specific disorder. Unwanted intrusive recurrent thoughts,
images or urges leading to distress or Consider obsessive
Coexisting psychiatric discomfort and/or excessive, ritualised compulsive disorder
disorders compulsive responses
Anxiety may be a symptom of, or coexist
Figure 1. Differential diagnosis of anxiety disorders
with, another underlying psychiatric
Reprinted from Australian Family Physician Vol. 40, No. 6, JUNE 2011 371