ENT
Seán Keenan
2022
,Otalgia
Description
The cause of otalgia is often non-otological (50 % of cases). Sources of referred pain (see table below) e.g. teeth and
throat are common.
Otitis Externa (OE)
Presentation Investigations
- Core: Ear pain on tragus; Itch; Scaling; Discharge - Otoscopy: Red, swollen, or eczematous canal
- Mild: Scaly skin; Non-swollen auditory canal Management
- Mod: Pain; Narrowed auditory canal; Discharge - 1L: Topical Abx ± Steroid; Ciprofloxacin if DM
- Severe: Auditory canal is occluded - NB: Avoid Aminoglycosides if tympanic perf.
- Brighton grading: Quantifies severity (see table) - 2L: Oral Abx (Flucloxacillin)
Causes - Severe: Al(CH3COOH) Ear wick prevents occlusion
- Infx: P. aeruginosa (Esp. in DM); S. aureus; Fungal - Unresponsive: Refer to ENT if Abx unresponsive
- Derm: Seborrheic dermatitis; Contact dermatitis Complications
- Risks: Swimming; Q-tips; Hearing aids - Malignant OE: ↑ risk of cancer or necrosis
Brighton Scoring system for quantifying severity of OE
Brighton Grade Description
Localised canal inflammationwith mild pain
I No hearing loss
Tympanic membrane visible
Debris in ear canal (not occluded)
II Erythmatous ear canal
Tympanic membrane partially obscured
Ear canal is occluded
III Ear canal is odematous and erythmatous
Tympanic membrane cannot be seen
Perichondritis and pinna cellulitis
IV Signs of systemic involvement
Tympanic membrane is obscured
Malignant / Necrotising OE
Description Investigations
- Incidence: 90 % of cases are in diabetics - CT Scan: Assesses spread
- Path: OE progression to temporal bone osteomyelitis Management
Causes - Refer: Urgent ENT referral
- Common: P. aeruginosa - Surgery: Debridement
- Other: Proteus; Klebsiella - Abx: Systemic Abx (anti-pseudomonal)
Barotrauma
Description Management
- Path: If eustachian tube becomes occluded - Lifestyle: No flying with an URTI (aerosinusitis)
- NB: Middle ear cannot equalise leading to damage - Nasal decongestants: Xylometazoline
Presentation - Supportive: Effusions clear spontaneously
- Initial: Severe pain; Occurs during descent
- Repeated: Transudate; Hemotympanum
TMJ Dysfunction
Presentation Management
- Features: Earache; Chronic facial pain - Reassurance: Usually resolves spontaneously
- NB: Tender open jaw; Pterygoid trigger points - Analgesia: NSAIDs; Paracetamol
,Discharge of the Ear and Otitis Media (OM)
Description
Risk factors for OM include: URTI; Bottle-feeding; passive smoking; pacifier adenoids; asthma; cleft palate; GORD.
Acute Otitis Media (AOM)
Description Causes
- Path: Typically occurs secondary to viral URTI - 2o Infx: Haemophilus; Pneumococcus; Moraxella
Presentation - Other: Streptococcus pneumoniae
- Features: Otalgia; Fever; Vomiting; Otorrhoea Management
- NB: Pain is relieved by perforation - Basic: Analgesia offers pain relief
- Severe: Erythematous swelling behind ear - Abx: If sx last >4 days; Systemic upset; Discharge
- Child: Ear tugging; Viral URTI may precede - NB: ↓ Immunity; Bilateral in <2 YO; <3 MO
Investigations - 1L: Amoxicillin 5-7 d; Macrolide if allergic
- Otoscope Exam - Perf: Heals within 6-8 wks; Avoid swimming
o Perf: Tympanic membrane Bulges ➔ Perforation Complications
o Discharge: Purulent discharge in perf - Common: Mastoiditis
o Mobility: Difficult to mobilise scope - Rare: Meningitis; Labyrinthitis; CHL; CNVII Palsy
o NB: Malleolus and Light reflex point anteriorly - Cc: Glue ear; Mastoiditis; Meningitis; CNVII Palsy
- Other tests Prognosis
o Labs: CRP; MC&S on discharge - Good: 60 % resolve within 24 hrs
o Imaging: CT if mastoiditis >24 hours
Chronic Otitis Media (COM)
Presentation Management
- Recurrent Infx: Tympanic membrane perforation - Abx: Topical; Systemic antibiotics
- Features: Otalgia; Otorrhoea; Hearing loss - Surgery: Myringoplasty; Mastoidectomy
- Chronic Serous OM: Serous otorrhoea Complications
- Chronic Suppurative OM: Purulent otorrhoea - Cholesteatoma: See below
Cholesteatoma
Description Investigations
- Incidence: Occurs 1:10k cases of COM - Otoscope: ‘Attic crust’; Upper part of ear drum
- Age: Peak age 5-15 YO Management
- Risk: Cleft palate ↑ risk 100-fold - Surgery: Mastoidectomy; Myringoplasty
- Path: Non-cancerous growth of squamous epithelium - Mastoidectomy: Debridement + Reconstruction
- NB: Tumour trapped in skull base ➔ Local destruction - Myringoplasty: Tympanic membrane graft
Presentation Complications
- Features: Malodorous discharge; CHL; Vertigo - Cc: Meningitis; Mastoiditis; CHL; CNVII palsy
- Other: Vertigo; CNVII; Cerebellopontine angle syn.
Mastoiditis
Description Management
- Path: Middle ear inflammation; Air cell destruction - Prevention: Abx in early OM ↓ risk
Presentation - Abx: IV Vancomycin + Ceftriaxone until MC&S
- Features: Severe otalgia; Fever; Otorrhoea - Surgery: Myringoplasty ± Mastoidectomy
- Mastoid: Erythema and Swelling of mastoid
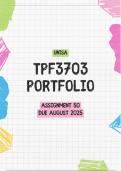
, Perforated tympanic membrane
CT scan of granulations (cholesteatoma) on left ear drum CT scan of Mastoiditis on left with no cholesteatoma
Seán Keenan
2022
,Otalgia
Description
The cause of otalgia is often non-otological (50 % of cases). Sources of referred pain (see table below) e.g. teeth and
throat are common.
Otitis Externa (OE)
Presentation Investigations
- Core: Ear pain on tragus; Itch; Scaling; Discharge - Otoscopy: Red, swollen, or eczematous canal
- Mild: Scaly skin; Non-swollen auditory canal Management
- Mod: Pain; Narrowed auditory canal; Discharge - 1L: Topical Abx ± Steroid; Ciprofloxacin if DM
- Severe: Auditory canal is occluded - NB: Avoid Aminoglycosides if tympanic perf.
- Brighton grading: Quantifies severity (see table) - 2L: Oral Abx (Flucloxacillin)
Causes - Severe: Al(CH3COOH) Ear wick prevents occlusion
- Infx: P. aeruginosa (Esp. in DM); S. aureus; Fungal - Unresponsive: Refer to ENT if Abx unresponsive
- Derm: Seborrheic dermatitis; Contact dermatitis Complications
- Risks: Swimming; Q-tips; Hearing aids - Malignant OE: ↑ risk of cancer or necrosis
Brighton Scoring system for quantifying severity of OE
Brighton Grade Description
Localised canal inflammationwith mild pain
I No hearing loss
Tympanic membrane visible
Debris in ear canal (not occluded)
II Erythmatous ear canal
Tympanic membrane partially obscured
Ear canal is occluded
III Ear canal is odematous and erythmatous
Tympanic membrane cannot be seen
Perichondritis and pinna cellulitis
IV Signs of systemic involvement
Tympanic membrane is obscured
Malignant / Necrotising OE
Description Investigations
- Incidence: 90 % of cases are in diabetics - CT Scan: Assesses spread
- Path: OE progression to temporal bone osteomyelitis Management
Causes - Refer: Urgent ENT referral
- Common: P. aeruginosa - Surgery: Debridement
- Other: Proteus; Klebsiella - Abx: Systemic Abx (anti-pseudomonal)
Barotrauma
Description Management
- Path: If eustachian tube becomes occluded - Lifestyle: No flying with an URTI (aerosinusitis)
- NB: Middle ear cannot equalise leading to damage - Nasal decongestants: Xylometazoline
Presentation - Supportive: Effusions clear spontaneously
- Initial: Severe pain; Occurs during descent
- Repeated: Transudate; Hemotympanum
TMJ Dysfunction
Presentation Management
- Features: Earache; Chronic facial pain - Reassurance: Usually resolves spontaneously
- NB: Tender open jaw; Pterygoid trigger points - Analgesia: NSAIDs; Paracetamol
,Discharge of the Ear and Otitis Media (OM)
Description
Risk factors for OM include: URTI; Bottle-feeding; passive smoking; pacifier adenoids; asthma; cleft palate; GORD.
Acute Otitis Media (AOM)
Description Causes
- Path: Typically occurs secondary to viral URTI - 2o Infx: Haemophilus; Pneumococcus; Moraxella
Presentation - Other: Streptococcus pneumoniae
- Features: Otalgia; Fever; Vomiting; Otorrhoea Management
- NB: Pain is relieved by perforation - Basic: Analgesia offers pain relief
- Severe: Erythematous swelling behind ear - Abx: If sx last >4 days; Systemic upset; Discharge
- Child: Ear tugging; Viral URTI may precede - NB: ↓ Immunity; Bilateral in <2 YO; <3 MO
Investigations - 1L: Amoxicillin 5-7 d; Macrolide if allergic
- Otoscope Exam - Perf: Heals within 6-8 wks; Avoid swimming
o Perf: Tympanic membrane Bulges ➔ Perforation Complications
o Discharge: Purulent discharge in perf - Common: Mastoiditis
o Mobility: Difficult to mobilise scope - Rare: Meningitis; Labyrinthitis; CHL; CNVII Palsy
o NB: Malleolus and Light reflex point anteriorly - Cc: Glue ear; Mastoiditis; Meningitis; CNVII Palsy
- Other tests Prognosis
o Labs: CRP; MC&S on discharge - Good: 60 % resolve within 24 hrs
o Imaging: CT if mastoiditis >24 hours
Chronic Otitis Media (COM)
Presentation Management
- Recurrent Infx: Tympanic membrane perforation - Abx: Topical; Systemic antibiotics
- Features: Otalgia; Otorrhoea; Hearing loss - Surgery: Myringoplasty; Mastoidectomy
- Chronic Serous OM: Serous otorrhoea Complications
- Chronic Suppurative OM: Purulent otorrhoea - Cholesteatoma: See below
Cholesteatoma
Description Investigations
- Incidence: Occurs 1:10k cases of COM - Otoscope: ‘Attic crust’; Upper part of ear drum
- Age: Peak age 5-15 YO Management
- Risk: Cleft palate ↑ risk 100-fold - Surgery: Mastoidectomy; Myringoplasty
- Path: Non-cancerous growth of squamous epithelium - Mastoidectomy: Debridement + Reconstruction
- NB: Tumour trapped in skull base ➔ Local destruction - Myringoplasty: Tympanic membrane graft
Presentation Complications
- Features: Malodorous discharge; CHL; Vertigo - Cc: Meningitis; Mastoiditis; CHL; CNVII palsy
- Other: Vertigo; CNVII; Cerebellopontine angle syn.
Mastoiditis
Description Management
- Path: Middle ear inflammation; Air cell destruction - Prevention: Abx in early OM ↓ risk
Presentation - Abx: IV Vancomycin + Ceftriaxone until MC&S
- Features: Severe otalgia; Fever; Otorrhoea - Surgery: Myringoplasty ± Mastoidectomy
- Mastoid: Erythema and Swelling of mastoid
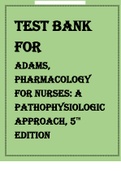
, Perforated tympanic membrane
CT scan of granulations (cholesteatoma) on left ear drum CT scan of Mastoiditis on left with no cholesteatoma