MSN 377 - Final Exam Study Guide with Answers
CARDIOVASCULAR SYSTEM DISORDERS
Hypertensive Emergency & Complications
Hours-days
>220/140
Clinical evidence of target organ disease
Complications: included in picture
Clinical Manifestations:
1. Hypertensive encephalopathy: HA, NV, seizures, confusion, coma, stroke
2. Renal Insufficiency: minor injury to renal failure
3. Cardiac Decompensation: unstable angina, MI, pulmonary edema, aortic dissection
Interprofessional Care:
ICU MAP monitoring (MAP = (SBP + 2DBP)÷3)
IV drugs Tx
Vasodilator: Sodium Nitroprusside (Nitropress)
Adrenergic Antagonist: phentolamine (Regitine)
ACE-I: enalapril (Vasotec)
Goal of care: slowly reduce BP (20-25% decrease in BP in first 1-2 hrs) except...
Aortic aneurysm → goal is <100-120 SBP quickly (to not rupture aneurysm)
Acute ischemic stroke → goal is to give thrombolytic HTN Complications
Hemorrhagic stroke → no thrombolytic!!
Dysrhythmias
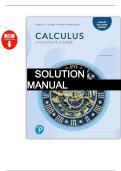
Waveform Meaning Interval (secs): only need to know bold/italicized durations
PR int. = 0.12 - 0.20 (3-5 small boxes)
P wave atrial depolarization → atrial systole 0.06 - 0.12
❤
atrial contraction to beginning of ventricle systole QRS int.= <0.12 (3 small boxes)
PR interval 0.12 - 0.20
(SA node to bundle of His) QT int. = 0.34 - 0.43 (8.5 - 10.75 small
QRS interval ventricular depolarization → ventricular systole < 0.12 (Note: 0.06-0.10 = normal; >0.12 = abnormal) boxes)
ST interval from S to beginning of T (normally isoelectric) 0.12
T wave ventricular repolarization → ventricular diastole 0.16
QT interval beginning of Q to end of T (start to end of V) 0.34 - 0.43 Intrinsic rates of the conduction
❤
U wave repolarization of Purkinje fibers or hypokalemia system:
SA node = 60-100 bpm
AV node = 40-60 bpm
Bundle of His/Purkinje = 20-40 bpm
MSN 377 - Final Exam Study Guide 1
, Cardioversion Indications Defibrillation Indications
VT with a pulse V-fib
SVT Pulseless VT
A-flutter w/ RVR
A-Fib
Cardiac & Anti-hypertensive Medications
Examples Indications MOA S/E Nursing Considerations
MSN 377 - Final Exam Study Guide 2
, Examples Indications MOA S/E Nursing Considerations
BBs Metoprolol Sinus tachycardia, PSVT, A-fib/-flutter, Blocks epinephrine (adrenaline) → Cold hands/feet, fatigue, bradycardia VS before admin (hold <60 HR)
PAC, PVC, HF, angina, MI ↓ HR/contractility → ↓ BP ✓
VS before admin, interactions with
Verapamil, Sinus tachycardia, PSVT, A-flutter, A-fib, Blocks Ca+ infux to heart → ↓ ✓
CCBs Amlodipine Prinzmetal angina contractility → ↓ BP Hypotension, AV block, bradycardia digoxin & grapefruit, caution w/ heart
block/failure
Blocks ACE from converting HA, dizziness, irritating cough, VS before admin; have 1:1000 Epi
✓
ACE-I Captopril HF, HTN, post-MI angiotensin I to angiotensin II → ↓ angioedema, tachycardia, available for angioedema; → ARBs
ALD secretion; ↓ AL/contractility hyperkalemia for those unable to tolerate ACE-I
VS for 1 full min; contraindicated in
✓
+ Inotropes Digoxin HF, A-fib/-flutter, ↑ contractility & ↓ HR NVD, bradycardia, HA, dizziness ventricular arrhythmias, ↓K/↑Ca → ↑
risk for toxicity (vision Δ’s: halo)
Dose-dependent: - 0.5-2 mcg/kg/min
Small dose → renal vasodilation; Irritation may occur at IV site, Monitor hemodynamic stability, BBs
+ Inotrope & = dopaminergic (renal perfusion) - 2-10
Dopamine Mod dose → cardiac β1 stim; High dyspnea, arrhythmia, hypotension, may counteract Tx effects, titrate to
vasopressor mcg/kg/min = inotropic - >10
dose → ⍺ stim → vasoconstrict angina, ECG Δ, palpitations BP
mcg/kg/min = vasoconstriction
HA, dizziness, abdominal cramps,
Bind & inhibit HMG-CoA reductase Monitor for cramps (muscle wasting),
Statins Atorvastatin HLD, CAD diarrhea, constipation, pancreatitis,
→ ↓ cholesterol syntehsis VS, Tx response: ↓ LDL/TG
rhabdomyolosis, rash
Hypokalemia may ↑ risk for digoxin
↓ reabsorption of Na/Cl in kidneys Hypotension, dry mouth, excessive
Diuretics (loop) Furosemide Edema, HTN toxicity; don’t give w/ aminoglycosides
and ↑ H2O, Na/Cl, Mg, K urination, E- abnormalities
(-mycins) d/t ototoxicity
CNS depression: Respiratory
Opioids Morphine Angina (ACS) ↓ pain/anxiety, ↓ PL/AL depression, euphoria, confusion, Naloxone for resp depression
sedation, hypotension, constipation
Coronary Artery Disease & Acute Coronary Syndrome
Goal of Tx: ↓ O2 demand or ↑ O2 supply
Acute Coronary Syndrome
Types of Angina:
Sustained ischemia → irreversible myocardial cell death (thrombus in 80-90% of
1. Stable (Classic) Angina: most common cases) → pt’s have to deal with sequelae for rest of life as a result of MI
a. Same pattern of onset, duration, and intensity of symptoms 20 mins w/o perfusion → heart muscle damage
b. Tx = NTG 4-6 hrs for entire thickness to become necrotic
2. Unstable (Progressive, Pre-infarction): Degree of altered cardiac function depends on area of myocardium affect (anterior vs
a. Unpredictable, ↑ frequency, provoked by minimal, no exercise, or at rest posterior, inferior vs lateral) and size of infarction (proximal vs distal)
b. ↑ risk of total occlusion → ↑ risk of MI Proximal thrombus affects more tissue; Distal affects less
c. Bedrest for 24-48 hrs tissue Anterior may be worse b/c this affects the LV
3. Prinzmetal’s (Coronary vasospasm):
STEMI NSTEMI
a. Occurs primarily at rest & may be triggered by smoking caused by occlusive thrombus caused by nonocclusive thrombus
b. H/o migraine or Raynaud’s d/t arterial vasospasm ST-elevation in leads facing area of infarction;
Non-ST elevation; ST depression instead or T
after a few days, T wave inverses and patho
c. Tx = CCBs wave inversion, but no patho Q wave
Q waves develop
Emergency: thrombolytic (TPA) or cath lab Non urgent cath lab (within 12-72 hrs); no
intervention thrombolytic
Artery opened within 90 mins (PCI or
May or may not develop ST-T wave changes
thrombolytic) to limit infarct size
Complications of MI
1. Dysrhythmias 6. Pericarditis: can occur 2-3 days post MI; may result in cardiac
tamponade (excess fluid in the pericardial sac AMB pericardial friction rub)
2. Heart failure: when pumping power of heart is diminished; subtle or severe
→ ↓ LV filling/emptying → HF
3. Cardiogenic shock: occurs less often w/ PCI or thromboytic; severe LV failure
CP and ECG changes (in ST segment of all leads)
Requires aggressive management
Tx = high dose ASA or sitting up & leaning over
4. Papillary muscle dysfunction or rupture: life-threatening d/t pulm edema;
Note: No steroids or anti-inflammatories (b/c they can impair scar
→ mitral valve regurgitation → aggravates an already compromised LV →
tissue formation) → only ASA!!
rapid deterioration
7. Dressler syndrome: can occur 1-8 weeks post MI;
Tx = Nitroprusside to reduce afterload
Pericarditis w/ fever & effusion (fluid accumulation; if lots → tamponade)
5. LV aneurysm (myocardial wall thins/bulges during contraction) → LV rupture,
HF, dysrhythmias, & angina Pericardial CP, friction rub, effusion
Arthralgia
Tx = high dose ASA
Rheumatic Heart Disease Prevention
Rheumatic Fever (RF): acute inflammatory disease of heart potentially involving all layers (pancarditis)
Complication of delayed group A streptococcal pharyngitis
MSN 377 - Final Exam Study Guide 3
CARDIOVASCULAR SYSTEM DISORDERS
Hypertensive Emergency & Complications
Hours-days
>220/140
Clinical evidence of target organ disease
Complications: included in picture
Clinical Manifestations:
1. Hypertensive encephalopathy: HA, NV, seizures, confusion, coma, stroke
2. Renal Insufficiency: minor injury to renal failure
3. Cardiac Decompensation: unstable angina, MI, pulmonary edema, aortic dissection
Interprofessional Care:
ICU MAP monitoring (MAP = (SBP + 2DBP)÷3)
IV drugs Tx
Vasodilator: Sodium Nitroprusside (Nitropress)
Adrenergic Antagonist: phentolamine (Regitine)
ACE-I: enalapril (Vasotec)
Goal of care: slowly reduce BP (20-25% decrease in BP in first 1-2 hrs) except...
Aortic aneurysm → goal is <100-120 SBP quickly (to not rupture aneurysm)
Acute ischemic stroke → goal is to give thrombolytic HTN Complications
Hemorrhagic stroke → no thrombolytic!!
Dysrhythmias
Waveform Meaning Interval (secs): only need to know bold/italicized durations
PR int. = 0.12 - 0.20 (3-5 small boxes)
P wave atrial depolarization → atrial systole 0.06 - 0.12
❤
atrial contraction to beginning of ventricle systole QRS int.= <0.12 (3 small boxes)
PR interval 0.12 - 0.20
(SA node to bundle of His) QT int. = 0.34 - 0.43 (8.5 - 10.75 small
QRS interval ventricular depolarization → ventricular systole < 0.12 (Note: 0.06-0.10 = normal; >0.12 = abnormal) boxes)
ST interval from S to beginning of T (normally isoelectric) 0.12
T wave ventricular repolarization → ventricular diastole 0.16
QT interval beginning of Q to end of T (start to end of V) 0.34 - 0.43 Intrinsic rates of the conduction
❤
U wave repolarization of Purkinje fibers or hypokalemia system:
SA node = 60-100 bpm
AV node = 40-60 bpm
Bundle of His/Purkinje = 20-40 bpm
MSN 377 - Final Exam Study Guide 1
, Cardioversion Indications Defibrillation Indications
VT with a pulse V-fib
SVT Pulseless VT
A-flutter w/ RVR
A-Fib
Cardiac & Anti-hypertensive Medications
Examples Indications MOA S/E Nursing Considerations
MSN 377 - Final Exam Study Guide 2
, Examples Indications MOA S/E Nursing Considerations
BBs Metoprolol Sinus tachycardia, PSVT, A-fib/-flutter, Blocks epinephrine (adrenaline) → Cold hands/feet, fatigue, bradycardia VS before admin (hold <60 HR)
PAC, PVC, HF, angina, MI ↓ HR/contractility → ↓ BP ✓
VS before admin, interactions with
Verapamil, Sinus tachycardia, PSVT, A-flutter, A-fib, Blocks Ca+ infux to heart → ↓ ✓
CCBs Amlodipine Prinzmetal angina contractility → ↓ BP Hypotension, AV block, bradycardia digoxin & grapefruit, caution w/ heart
block/failure
Blocks ACE from converting HA, dizziness, irritating cough, VS before admin; have 1:1000 Epi
✓
ACE-I Captopril HF, HTN, post-MI angiotensin I to angiotensin II → ↓ angioedema, tachycardia, available for angioedema; → ARBs
ALD secretion; ↓ AL/contractility hyperkalemia for those unable to tolerate ACE-I
VS for 1 full min; contraindicated in
✓
+ Inotropes Digoxin HF, A-fib/-flutter, ↑ contractility & ↓ HR NVD, bradycardia, HA, dizziness ventricular arrhythmias, ↓K/↑Ca → ↑
risk for toxicity (vision Δ’s: halo)
Dose-dependent: - 0.5-2 mcg/kg/min
Small dose → renal vasodilation; Irritation may occur at IV site, Monitor hemodynamic stability, BBs
+ Inotrope & = dopaminergic (renal perfusion) - 2-10
Dopamine Mod dose → cardiac β1 stim; High dyspnea, arrhythmia, hypotension, may counteract Tx effects, titrate to
vasopressor mcg/kg/min = inotropic - >10
dose → ⍺ stim → vasoconstrict angina, ECG Δ, palpitations BP
mcg/kg/min = vasoconstriction
HA, dizziness, abdominal cramps,
Bind & inhibit HMG-CoA reductase Monitor for cramps (muscle wasting),
Statins Atorvastatin HLD, CAD diarrhea, constipation, pancreatitis,
→ ↓ cholesterol syntehsis VS, Tx response: ↓ LDL/TG
rhabdomyolosis, rash
Hypokalemia may ↑ risk for digoxin
↓ reabsorption of Na/Cl in kidneys Hypotension, dry mouth, excessive
Diuretics (loop) Furosemide Edema, HTN toxicity; don’t give w/ aminoglycosides
and ↑ H2O, Na/Cl, Mg, K urination, E- abnormalities
(-mycins) d/t ototoxicity
CNS depression: Respiratory
Opioids Morphine Angina (ACS) ↓ pain/anxiety, ↓ PL/AL depression, euphoria, confusion, Naloxone for resp depression
sedation, hypotension, constipation
Coronary Artery Disease & Acute Coronary Syndrome
Goal of Tx: ↓ O2 demand or ↑ O2 supply
Acute Coronary Syndrome
Types of Angina:
Sustained ischemia → irreversible myocardial cell death (thrombus in 80-90% of
1. Stable (Classic) Angina: most common cases) → pt’s have to deal with sequelae for rest of life as a result of MI
a. Same pattern of onset, duration, and intensity of symptoms 20 mins w/o perfusion → heart muscle damage
b. Tx = NTG 4-6 hrs for entire thickness to become necrotic
2. Unstable (Progressive, Pre-infarction): Degree of altered cardiac function depends on area of myocardium affect (anterior vs
a. Unpredictable, ↑ frequency, provoked by minimal, no exercise, or at rest posterior, inferior vs lateral) and size of infarction (proximal vs distal)
b. ↑ risk of total occlusion → ↑ risk of MI Proximal thrombus affects more tissue; Distal affects less
c. Bedrest for 24-48 hrs tissue Anterior may be worse b/c this affects the LV
3. Prinzmetal’s (Coronary vasospasm):
STEMI NSTEMI
a. Occurs primarily at rest & may be triggered by smoking caused by occlusive thrombus caused by nonocclusive thrombus
b. H/o migraine or Raynaud’s d/t arterial vasospasm ST-elevation in leads facing area of infarction;
Non-ST elevation; ST depression instead or T
after a few days, T wave inverses and patho
c. Tx = CCBs wave inversion, but no patho Q wave
Q waves develop
Emergency: thrombolytic (TPA) or cath lab Non urgent cath lab (within 12-72 hrs); no
intervention thrombolytic
Artery opened within 90 mins (PCI or
May or may not develop ST-T wave changes
thrombolytic) to limit infarct size
Complications of MI
1. Dysrhythmias 6. Pericarditis: can occur 2-3 days post MI; may result in cardiac
tamponade (excess fluid in the pericardial sac AMB pericardial friction rub)
2. Heart failure: when pumping power of heart is diminished; subtle or severe
→ ↓ LV filling/emptying → HF
3. Cardiogenic shock: occurs less often w/ PCI or thromboytic; severe LV failure
CP and ECG changes (in ST segment of all leads)
Requires aggressive management
Tx = high dose ASA or sitting up & leaning over
4. Papillary muscle dysfunction or rupture: life-threatening d/t pulm edema;
Note: No steroids or anti-inflammatories (b/c they can impair scar
→ mitral valve regurgitation → aggravates an already compromised LV →
tissue formation) → only ASA!!
rapid deterioration
7. Dressler syndrome: can occur 1-8 weeks post MI;
Tx = Nitroprusside to reduce afterload
Pericarditis w/ fever & effusion (fluid accumulation; if lots → tamponade)
5. LV aneurysm (myocardial wall thins/bulges during contraction) → LV rupture,
HF, dysrhythmias, & angina Pericardial CP, friction rub, effusion
Arthralgia
Tx = high dose ASA
Rheumatic Heart Disease Prevention
Rheumatic Fever (RF): acute inflammatory disease of heart potentially involving all layers (pancarditis)
Complication of delayed group A streptococcal pharyngitis
MSN 377 - Final Exam Study Guide 3