Exercise Psychology
1. Exercise Behaviour Change Theories and Interventions
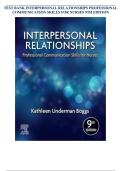
Theory of Reasoned Action: (Ajzen and Fishbein, 1980)
Behaviours under our control (volitional) such as exercise, are best predicted by a person’s
intention. A persons intention consists of their attitude to the behaviour and the subjective
norms associated with the behaviour.
Behavioural beliefs – thoughts regarding the behaviour.
Overcome evaluation – perceived outcome of behaviour.
Normative beliefs – what I think others would want/expect me to do.
Motivation to comply – how important it is to me to do what I think other expect.
The theory does have some limiting factors as it’s limited to predictive behaviour under our
control. Additional factors other than intention such as social and structural are important
and the complex interaction of factors are difficult to predict.
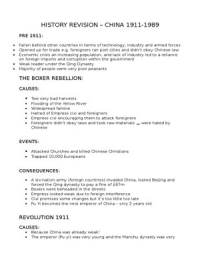
Theory of Planned Behaviour: (Ajzen and Madden, 1986)
Ajzen revised the previous model to increase its predictive power and counteract its
limitations. He added a perceived behavioural control component.
Perceived behavioural control consists of two processes: perceived difficulty of the
behaviour and perceived capability for the individual to accomplish the behaviour. It’s
effectively self-efficacy.
Strengths – intention and behaviour are strongly correlated. There are clear definitions of
the constructs and it’s a parsimonious model (simple and explains a lot of variance.)
,Weaknesses – most research is correlational and there is an intention-behaviour gap. It also
ignores other factors such as emotions and can be argued as being too parsimonious.
Self-determination Theory: Deci and Ryan, 1980
This is a humanistic theory of motivated behaviour. It identifies two main types of motivated
behaviour (intrinsic and extrinsic.)
Intrinsic – exercising for satisfaction, enjoyment, and/or accomplishment.
Extrinsic – exercising for instrumental reasons, rewards, social approval and to avoid
disapproval. Extrinsic motivation is differentiated based on its level of autonomy.
Examples:
1. Amotivation – no motivation.
2. External regulation – external rewards and punishment.
3. Introjected regulation – internal rewards and punishment.
4. Identified regulation – recognised importance.
5. Integrated regulation – congruent with self and values.
6. Intrinsic regulation – because of enjoyment and satisfaction.
Basic Psychological Needs (Ryan, 1995) – basic psychological needs represent the building
blocks for developing autonomous forms of motivation.
Autonomy – choice, volition and exercise aligned with sense of self.
Competence – success and failure during exercise with feedback from others.
Relatedness – feeling connected, loved and cared for.
Social environments which are supportive of the basic psychological needs are key (need
supportive environments. These environments promote autonomy, competence and
relatedness.
Need supportive environments are thought to explain a large amount of individual
differences in peoples motivation.
Goal Contents (Kasser and Ryan, 1996) – goal content is the outcome pursued by engaging
in the behaviour. It can be differentiated on the extent to which the goal is likely to increase
autonomous motivation.
, People often have multiple goals, and the quality and strength of these goals determine the
impact on basic psychological needs. Goals can be both intrinsic and extrinsic.
Causality Orientations (Deci and Ryan, 1985) – causality orientations are dispositional
tendencies in motivational and behavioural patterns. People might be predisposed to
intrinsic and extrinsic motivation and amotivation (unresponsive to intrinsic/extrinsic
factors.)
Self-determination Theory: (Ryan, Williams, Patrick and Deci, 2009)
Developing Exercise Interventions:
Intervention – a health intervention is an act performed for, with or on behalf of a person or
population whose purpose is to assess, improve, maintain, promote or modify health,
functioning or health conditions. Good interventions are:
1. Affordable – can everyone afford it?
2. Practicable – can it be delivered to everyone?
3. Effective – will it substantially change behaviour?
4. Acceptable – is it publicly/professionally/politically acceptable?
5. Safe and equitable – does it have unwanted side effects/consequences? Will it
reduce/increase the disparities in health/well-being.
Designing behaviour change interventions typically involves firstly determining the broad
approach which will be used and then working on the specifics of the intervention (Mitchie
et al., 2011.)
Broad approach – underpinning theory, model or framework.
Specifics – behaviour change techniques.
Broad Approach: Theory Led Interventions
Interventions should draw on theories of behaviour change in their development
because theories identify what should be focused on.
Without a theoretical basis there is little guidance on intervention design.
1. Exercise Behaviour Change Theories and Interventions
Theory of Reasoned Action: (Ajzen and Fishbein, 1980)
Behaviours under our control (volitional) such as exercise, are best predicted by a person’s
intention. A persons intention consists of their attitude to the behaviour and the subjective
norms associated with the behaviour.
Behavioural beliefs – thoughts regarding the behaviour.
Overcome evaluation – perceived outcome of behaviour.
Normative beliefs – what I think others would want/expect me to do.
Motivation to comply – how important it is to me to do what I think other expect.
The theory does have some limiting factors as it’s limited to predictive behaviour under our
control. Additional factors other than intention such as social and structural are important
and the complex interaction of factors are difficult to predict.
Theory of Planned Behaviour: (Ajzen and Madden, 1986)
Ajzen revised the previous model to increase its predictive power and counteract its
limitations. He added a perceived behavioural control component.
Perceived behavioural control consists of two processes: perceived difficulty of the
behaviour and perceived capability for the individual to accomplish the behaviour. It’s
effectively self-efficacy.
Strengths – intention and behaviour are strongly correlated. There are clear definitions of
the constructs and it’s a parsimonious model (simple and explains a lot of variance.)
,Weaknesses – most research is correlational and there is an intention-behaviour gap. It also
ignores other factors such as emotions and can be argued as being too parsimonious.
Self-determination Theory: Deci and Ryan, 1980
This is a humanistic theory of motivated behaviour. It identifies two main types of motivated
behaviour (intrinsic and extrinsic.)
Intrinsic – exercising for satisfaction, enjoyment, and/or accomplishment.
Extrinsic – exercising for instrumental reasons, rewards, social approval and to avoid
disapproval. Extrinsic motivation is differentiated based on its level of autonomy.
Examples:
1. Amotivation – no motivation.
2. External regulation – external rewards and punishment.
3. Introjected regulation – internal rewards and punishment.
4. Identified regulation – recognised importance.
5. Integrated regulation – congruent with self and values.
6. Intrinsic regulation – because of enjoyment and satisfaction.
Basic Psychological Needs (Ryan, 1995) – basic psychological needs represent the building
blocks for developing autonomous forms of motivation.
Autonomy – choice, volition and exercise aligned with sense of self.
Competence – success and failure during exercise with feedback from others.
Relatedness – feeling connected, loved and cared for.
Social environments which are supportive of the basic psychological needs are key (need
supportive environments. These environments promote autonomy, competence and
relatedness.
Need supportive environments are thought to explain a large amount of individual
differences in peoples motivation.
Goal Contents (Kasser and Ryan, 1996) – goal content is the outcome pursued by engaging
in the behaviour. It can be differentiated on the extent to which the goal is likely to increase
autonomous motivation.
, People often have multiple goals, and the quality and strength of these goals determine the
impact on basic psychological needs. Goals can be both intrinsic and extrinsic.
Causality Orientations (Deci and Ryan, 1985) – causality orientations are dispositional
tendencies in motivational and behavioural patterns. People might be predisposed to
intrinsic and extrinsic motivation and amotivation (unresponsive to intrinsic/extrinsic
factors.)
Self-determination Theory: (Ryan, Williams, Patrick and Deci, 2009)
Developing Exercise Interventions:
Intervention – a health intervention is an act performed for, with or on behalf of a person or
population whose purpose is to assess, improve, maintain, promote or modify health,
functioning or health conditions. Good interventions are:
1. Affordable – can everyone afford it?
2. Practicable – can it be delivered to everyone?
3. Effective – will it substantially change behaviour?
4. Acceptable – is it publicly/professionally/politically acceptable?
5. Safe and equitable – does it have unwanted side effects/consequences? Will it
reduce/increase the disparities in health/well-being.
Designing behaviour change interventions typically involves firstly determining the broad
approach which will be used and then working on the specifics of the intervention (Mitchie
et al., 2011.)
Broad approach – underpinning theory, model or framework.
Specifics – behaviour change techniques.
Broad Approach: Theory Led Interventions
Interventions should draw on theories of behaviour change in their development
because theories identify what should be focused on.
Without a theoretical basis there is little guidance on intervention design.