9/6/24, 4:07 Electronic Fetal
PM Monitoring
Electronic Fetal Monitoring
Assessment of fetal heart rate (FHR) and assessment of fetal tolerance to
labor Two points of data – FHR and uterine contractions
With each contraction, there is a temporary, transient reduction in maternal blood flow to fetus,
electronic fetal monitoring provides visual picture of how fetus is responding to stress of
contractions
The RN is responsible to read and interpret the FHR pattern/contractions to evaluate fetal well-
being 2 types of monitoring: Internal vs. External
Contraction monitor at top of fundus
Always check that you are tracing baby (moms pulse vs reading)
External Internal
intermittent Continuous **Can only be continuous!!
Low risk, early active labor, ** have to have rupture of membranes (ROM)
labor, non- preeclampsia (treated - Internal monitors placed by physician
medicated, no with medications – or CNM
rupture Pitocin or Internal assessment of contractions & FHR
Assess fetal HR magnesium), higher Done because external monitoring is not
- Handheld risk pregnancies, adequate
doppler twins
- Ultrasound Assess contractions: Done when labor is not progressing, for accurate
stethoscope Tocotransducer dosage of Pitocin
- Fetoscope - Frequency
Assess before/during/ - Duration Intrauterine pressure catheter (IUPC)
after a contraction in - NOT intensity assesses contractions
labor Assess fetal HR: - Catheter sits between uterine wall
- Use palpation Ultrasound doppler and fetus, connects to monitor
to assess for - Baseline - Strength expressed as Montevideo units
contraction - Variability (MVU)
Seen a lot with - Presence of - Assess intensity (strength) of
midwife care accelerations contraction Only way to determine the
or strength/intensity of a contraction, and
deceleration external monitor cannot
Of every 15 minutes, Fetal scalp electrode (FSE)
we take 10 minutes assesses FHR
and document - Spiral electrode placed into
contractions vs fetal fetal presenting part
HR - Cable from electrode to
monitor Risks: bleeding, hematoma,
infection, Caution in patients (mom)
Monitor strip basics with HIV
about:bl 1
, 9/6/24, 4:07 Electronic Fetal
PM Monitoring
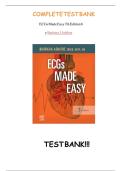
Top line Bottom line Vertical line
FHR tracing Uterine contraction tracing Time (10 seconds)
*The intervals between vertical lines represents one minute
Fetal Heart Rate Uterine Contractions
FHR baseline Frequency
Variability Intensity
Presence of accelerations and decelerations - Mild = nose
- Moderate = chin
- Strong = forehead
Duration
- Visual representation of the FHR and the maternal contraction pattern
- Information about fetal oxygenation & changes in FHR
- FHR pattern changes can indicate fetal hypoxemia – the most common etiology of
fetal injury/death
- Optimal fetal surveillance during labor to detect FHR changes combined with early
interventions can help prevent fetal injury/death
Normal baseline 110 – 160 bpm
- Assess over 10 minutes to determine baseline (at least 2 minutes of identifiable baseline –
otherwise baseline may be indeterminate)
- Round to nearest 5 bpm
Bradycardia Tachycardia
Less than 110 bpm Over 160 bpm
Causes: late fetal hypoxemia, maternal Causes: maternal fever (most common), early
hypotension (may be from epidural), fetal hypoxemia, maternal dehydration
uterine rupture, placental abruption,
medication (opioids), maternal supine Intervention: requires additional assessment to
position determine cause – fluids
Fever = temperature check, Tylenol,
Can come from prolonged deceleration, only fix cold compress, increase fluids
is delivery
**mother will receive fluids before epidural to
prevent hypotension and bradycardia in the
fetus, if persists can give more fluids and/or epi
Intervention: Increase placental perfusion,
decrease uterine activity, correct
hypotension (position)
Variability – the push pull between the sympathetic and parasympathetic nervous system
*Absent, minimal, moderate, marked*
- The most important predictor of adequate fetal oxygenation and fetal reserve during labor
- Absent – no “push – pull”
- Minimal – baby may not be awake, so less variability. Could be from pain medications
(mg, staidol)
- Moderate variability indicates well developed and well oxygenated autonomic and CNS
o Good sign on fetal well-being
- Marked – goes over 25 bpm, not a huge deal but don’t like this too much
about:bl 2
PM Monitoring
Electronic Fetal Monitoring
Assessment of fetal heart rate (FHR) and assessment of fetal tolerance to
labor Two points of data – FHR and uterine contractions
With each contraction, there is a temporary, transient reduction in maternal blood flow to fetus,
electronic fetal monitoring provides visual picture of how fetus is responding to stress of
contractions
The RN is responsible to read and interpret the FHR pattern/contractions to evaluate fetal well-
being 2 types of monitoring: Internal vs. External
Contraction monitor at top of fundus
Always check that you are tracing baby (moms pulse vs reading)
External Internal
intermittent Continuous **Can only be continuous!!
Low risk, early active labor, ** have to have rupture of membranes (ROM)
labor, non- preeclampsia (treated - Internal monitors placed by physician
medicated, no with medications – or CNM
rupture Pitocin or Internal assessment of contractions & FHR
Assess fetal HR magnesium), higher Done because external monitoring is not
- Handheld risk pregnancies, adequate
doppler twins
- Ultrasound Assess contractions: Done when labor is not progressing, for accurate
stethoscope Tocotransducer dosage of Pitocin
- Fetoscope - Frequency
Assess before/during/ - Duration Intrauterine pressure catheter (IUPC)
after a contraction in - NOT intensity assesses contractions
labor Assess fetal HR: - Catheter sits between uterine wall
- Use palpation Ultrasound doppler and fetus, connects to monitor
to assess for - Baseline - Strength expressed as Montevideo units
contraction - Variability (MVU)
Seen a lot with - Presence of - Assess intensity (strength) of
midwife care accelerations contraction Only way to determine the
or strength/intensity of a contraction, and
deceleration external monitor cannot
Of every 15 minutes, Fetal scalp electrode (FSE)
we take 10 minutes assesses FHR
and document - Spiral electrode placed into
contractions vs fetal fetal presenting part
HR - Cable from electrode to
monitor Risks: bleeding, hematoma,
infection, Caution in patients (mom)
Monitor strip basics with HIV
about:bl 1
, 9/6/24, 4:07 Electronic Fetal
PM Monitoring
Top line Bottom line Vertical line
FHR tracing Uterine contraction tracing Time (10 seconds)
*The intervals between vertical lines represents one minute
Fetal Heart Rate Uterine Contractions
FHR baseline Frequency
Variability Intensity
Presence of accelerations and decelerations - Mild = nose
- Moderate = chin
- Strong = forehead
Duration
- Visual representation of the FHR and the maternal contraction pattern
- Information about fetal oxygenation & changes in FHR
- FHR pattern changes can indicate fetal hypoxemia – the most common etiology of
fetal injury/death
- Optimal fetal surveillance during labor to detect FHR changes combined with early
interventions can help prevent fetal injury/death
Normal baseline 110 – 160 bpm
- Assess over 10 minutes to determine baseline (at least 2 minutes of identifiable baseline –
otherwise baseline may be indeterminate)
- Round to nearest 5 bpm
Bradycardia Tachycardia
Less than 110 bpm Over 160 bpm
Causes: late fetal hypoxemia, maternal Causes: maternal fever (most common), early
hypotension (may be from epidural), fetal hypoxemia, maternal dehydration
uterine rupture, placental abruption,
medication (opioids), maternal supine Intervention: requires additional assessment to
position determine cause – fluids
Fever = temperature check, Tylenol,
Can come from prolonged deceleration, only fix cold compress, increase fluids
is delivery
**mother will receive fluids before epidural to
prevent hypotension and bradycardia in the
fetus, if persists can give more fluids and/or epi
Intervention: Increase placental perfusion,
decrease uterine activity, correct
hypotension (position)
Variability – the push pull between the sympathetic and parasympathetic nervous system
*Absent, minimal, moderate, marked*
- The most important predictor of adequate fetal oxygenation and fetal reserve during labor
- Absent – no “push – pull”
- Minimal – baby may not be awake, so less variability. Could be from pain medications
(mg, staidol)
- Moderate variability indicates well developed and well oxygenated autonomic and CNS
o Good sign on fetal well-being
- Marked – goes over 25 bpm, not a huge deal but don’t like this too much
about:bl 2