DERMATOLOGY Pathology:
Rosacea
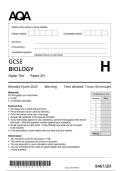
ROSACEA:
- What is it?:
o Predominantly a Facial Rash easily confused with Acne.
o = Pustules and Papular Rash on Face
o Typically a Disease of Middle Age (30-40yrs).
- Aetiology:
o Unknown
o (But Familial Association)
o Aggregating Factors:
③ Heat and steam
③ Hot, spicy food
③ Alcohol consumption
③ Emotional stress
③ Sun exposure
- Presentation:
o Wide Variation in Severity
o Initial Signs:
③ Tendency to Flush easily + Burning/Stinging/Itching.
o Distinguishing Features:
③ Facial Flushing (Erythema)
③ Dilated, visible Capillaries (Telangiectasia)
③ Papules
③ Pustules
③ But NOT Comedoens
o If Severe:
③ Disfiguring Facial Rash
③ + Bulbous Enlargement of the Nose
③ Possible Facial Oedema
o NO Comedones (:. NOT Acne)
o Does not cause Scarring
o Very Chronic (Not Self Limiting – May last for many years)
o (NB: Often significant Psychosocial Impact – Eg. Depression)
- Diagnosis:
o Differential Diagnoses:
③ Acne (has all features + Comedones)
③ Sun Damage (has Telangiectasia, but No other Features)
③ Lupus Erythematosus (Have Telangiectasia & Erythema, But NO Pustules or Papules)
③ Menopause (Flushing)
- Treatment:
o Avoidance of Aggravating Factors
o Similar Treatment to Acne.
, ③ Antibiotics (Some have Anti-Inflammatory Effects)
③ Retinoids
o Laser surgery (for Telangiectasia & Erythema)
o Topical corticosteroids make rosacea worse and should never be used to treat it!
③ ⮴ Cause Perioral Dermatitis (Should NEVER be used in Rosacea)
www.MedStudentNotes.com
DERMATOLOGY Pathology:
Seborrhoeic Dermatitis
Seborrhoeic Dermatitis – 2 Forms:
ξ Infantile Seborrhoeic Dermatitis:
o Clinical Presentation:
③ Numerous Dermatoses in the 1st 3 Months of Life.
③ Erythematous but Non-Itchy Rash involving the face, scalp, neck, axillae and nappy area. The lesions are well defined and covered
in greasy scale.
ξ Adult Seborrhoeic Dermatitis:
o Clinical Presentation:
o Erythema and fine, greasy scale on the cheeks, nose and nasolabial folds.
o Scale and itching of the scalp and eyebrows.
DERMATOLOGY Pathology:
Skin Infections ʹ Bacterial
BACTERIAL SKIN INFECTIONS:
- Impetigo (AKA ͞School Scores͟):
o What is it?
③ Superficial Bacterial Skin Infection
③ Most Common in school kids
③ Very Contagious ʹ (Spread by Close Contact & Poor Hygeine)
③ Usually resolves slowly
o Organism:
③ Mostly Staphylococcus Aureus
③ Sometimes Streptococcus Pyogenes
ξ Can lead to Glomerulonephritis or Rheumatic Fever if iƚ͛Ɛ Sƚƌe Ɖ͘
③ Staph. Aureus (Bullous) - (Pic 1)
③ Streptococcus (Non-bullous) ʹ (Pic 2)
③
o Presentations:
③ Occur most commonly on face
③ Fragile vesicles rupture & crust
③ Can be confused with HSV
③ 1. Nonbullous/Crusted Impetigo:
ξ (Most common)
ξ Yellow crusts and erosions
ξ Itchy/Irritating (but not painful).
③ 2. Bullous impetigo:
Rosacea
ROSACEA:
- What is it?:
o Predominantly a Facial Rash easily confused with Acne.
o = Pustules and Papular Rash on Face
o Typically a Disease of Middle Age (30-40yrs).
- Aetiology:
o Unknown
o (But Familial Association)
o Aggregating Factors:
③ Heat and steam
③ Hot, spicy food
③ Alcohol consumption
③ Emotional stress
③ Sun exposure
- Presentation:
o Wide Variation in Severity
o Initial Signs:
③ Tendency to Flush easily + Burning/Stinging/Itching.
o Distinguishing Features:
③ Facial Flushing (Erythema)
③ Dilated, visible Capillaries (Telangiectasia)
③ Papules
③ Pustules
③ But NOT Comedoens
o If Severe:
③ Disfiguring Facial Rash
③ + Bulbous Enlargement of the Nose
③ Possible Facial Oedema
o NO Comedones (:. NOT Acne)
o Does not cause Scarring
o Very Chronic (Not Self Limiting – May last for many years)
o (NB: Often significant Psychosocial Impact – Eg. Depression)
- Diagnosis:
o Differential Diagnoses:
③ Acne (has all features + Comedones)
③ Sun Damage (has Telangiectasia, but No other Features)
③ Lupus Erythematosus (Have Telangiectasia & Erythema, But NO Pustules or Papules)
③ Menopause (Flushing)
- Treatment:
o Avoidance of Aggravating Factors
o Similar Treatment to Acne.
, ③ Antibiotics (Some have Anti-Inflammatory Effects)
③ Retinoids
o Laser surgery (for Telangiectasia & Erythema)
o Topical corticosteroids make rosacea worse and should never be used to treat it!
③ ⮴ Cause Perioral Dermatitis (Should NEVER be used in Rosacea)
www.MedStudentNotes.com
DERMATOLOGY Pathology:
Seborrhoeic Dermatitis
Seborrhoeic Dermatitis – 2 Forms:
ξ Infantile Seborrhoeic Dermatitis:
o Clinical Presentation:
③ Numerous Dermatoses in the 1st 3 Months of Life.
③ Erythematous but Non-Itchy Rash involving the face, scalp, neck, axillae and nappy area. The lesions are well defined and covered
in greasy scale.
ξ Adult Seborrhoeic Dermatitis:
o Clinical Presentation:
o Erythema and fine, greasy scale on the cheeks, nose and nasolabial folds.
o Scale and itching of the scalp and eyebrows.
DERMATOLOGY Pathology:
Skin Infections ʹ Bacterial
BACTERIAL SKIN INFECTIONS:
- Impetigo (AKA ͞School Scores͟):
o What is it?
③ Superficial Bacterial Skin Infection
③ Most Common in school kids
③ Very Contagious ʹ (Spread by Close Contact & Poor Hygeine)
③ Usually resolves slowly
o Organism:
③ Mostly Staphylococcus Aureus
③ Sometimes Streptococcus Pyogenes
ξ Can lead to Glomerulonephritis or Rheumatic Fever if iƚ͛Ɛ Sƚƌe Ɖ͘
③ Staph. Aureus (Bullous) - (Pic 1)
③ Streptococcus (Non-bullous) ʹ (Pic 2)
③
o Presentations:
③ Occur most commonly on face
③ Fragile vesicles rupture & crust
③ Can be confused with HSV
③ 1. Nonbullous/Crusted Impetigo:
ξ (Most common)
ξ Yellow crusts and erosions
ξ Itchy/Irritating (but not painful).
③ 2. Bullous impetigo: