Translational neuroscience
LES 1: Alzheimer’s and dementia from clinical perspective
(Engelborghs)
Dementia and Alzheimer's disease (AD): epidemiology
Since 2023: dementia = 1st cause of death in Belgium
develops dementia
As age is main risk factor and given ageing population, number of people with dementia is expected to have doubled in
2070
DEMENTIA = UMBRELLA
memory problems, spatial problems, .... are the symptoms but is not
the disease
people with dementia has 3 pilars
* cognitive pilar
* change of personality and behaviour
* functional deficits (activities of daily living become complex,
become dependent on others to survive)
if you think of dementia you think of memory problems and for AD
this is true this is the most common symptom but for FTLD the most
common symptom is behavioural problem
ALZHEIMER’S DISEASE (AD): THE AMYLOID CASCADE HYPOTHESIS
1) The formation of ameloid
plaques is the first thing that happens
in the brain
ameloid precursor protein produces
42 AZ ameloid beta protein which is
insoluble and then it starts clitting
together forming deposits in the brain
= ameloid plaques
Has a dense ameloid nucleus
In between the neurons
2) tau protein is the basis of the
cytoskeleton of neurons (for
structural reasons but also for
transport of neurotransmitters)
tau gets hyperphosphorylated and tau loses its function and forms aggregates and deposits of hyperphosphorylated tau =
neurofibrillary tangles
Within the neurons
3) Degeneration of neurons + number of synapses start decreasing (=synaptic degeneration)
This correlates with the cognitive decline in neurons
4) Loss of neurons themselves and schrinkage of the brain
Brain schrinkage is normal in aging but in AD it starts earlier and is more progressive
hippocampus is a structure that is important to transfer info to your memory
atrofie is max in hippocampus -> biomarker for diagnostic + recent memory problems
loss of neurons themselves and the brain schrinks = atrofie
1
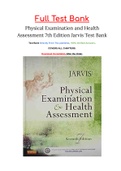
,sequence of spread of neurofibrillary tangles
the darker the red, the higher the intensity of neurofibrillary
tangles
ameloid plaque are more localised so this doens't affect the
whole brain as compaired to this
MCI: people with for eg memory problems but for the rest are
normal because they don't have symptoms in the 3 pilars of
dementia
do all people with AD have dementia? NO, the first ameloid
plaques occure 20 years before the symptoms so brain 1 has
AD but no dementia
The Alzheimer continuum
you spend the majority of the disease in the preclinical stage
→ building up the disease without showing symptoms
The first diagnosis is the mild cognitive impairment -> new
methods are focused on diagnosis early dementia or MCI and
treating this
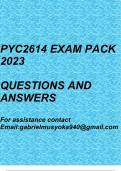
How is AD diagnosed?
make use of markers of the disease → coloured curves
are different markers we use in clinical practice
they move from normal to abnormal throughout the
different stages of the disease
ADL = activities of daily living
Functional deficits
MCI have no deficits but everyone with dementia
has deficits in ADL → every consultation of
someone with MCI we ask about deficits in ADL
and once there are deficits the person has
developed dementia
Neuropsychologists takes the history of patient & family to detect other causes of cognitive problems -> sleep problems
can also cause memory problems (is a complete other cause than dementia). Then he starts testing the different cognitive
functions to cover all cognitive domains → you have norms for these domains (“the mean score for this patient must be
X”)
Result of such test is “the cognitive function are normal for this age” or “has MCI” or he can specify for a specific domain
like everything is good but memory is affected -> can give a disease stage
Cornerstone of the diagnosis of dementia and AD. Can’t diagnose it without this
Biomarkers alone can give an incorrect diagnosis. Neuropsychologic exam should always be performed -> time consuming
and expensive
NEUROPSYCHOLOGICAL EXAMINATION
Requires neuropsychologist
Time-consuming: 2h of testing, 1h of data analysis and writing report Reimbursed once in a life-time for about half of the
cost price
Only AD biomarker testing if objective cognitive deficits in a consented patients (right to know versus right to refuse
diagnosis of an incurable disease)
2
,Thus:
1. Neuropsychology = required!
2. Neuropsychology = bottle neck in diagnostic work-up given number of neuropsychologists and reimbursement
MRI IN AD: HIPPOCAMPAL ATROPHY (blue curve)
Hippocampus is a small 3D structure that can be hard in the early
stages of the disease to diagnose the atrofie → that’s why we
nowadays use AI
develop AI based software pipeline and help with the analysis of
MR images for brain diseases
now incorporated in routine → after 30 min you get a report with
the brain volume in total, volumes of different parts of the brain
and the comparison with what is normal for that age
helps to detect hippocampal degeneration in earliest stages
CSF BIOMARKERS
red: ameloid curve = the first thing that happens in the brain
Ameloid PET to look at the ameloid deposits in the brain →
expensive (depending on the tracer + health care doesn’t pay
in Belgium) + capacity of PET scans is limited
Not used in clinical practice
Instead we do a lumbar puncture to withdraw CSF that finds
its origin in the brain so the metabolism of the brain is
reflected in the CSF → proteins linked to AD can be found
Ameloid beta of 42 az (main constituent of ameloid
plaques) → levels in the brain get lower in case of AD
Phosphorylated tau (main component of neurofibrillary
tangles) → increased in AD
Total tau fraction (composed of normal and
hyperphosphorylated tau) → increases in AD because
of neurodegeneration
Lumbar puncture is only to help diagnose and cannot help you with the severity of the disease → neuropsychological
exam gives severity
So one lumbar puncture gives the whole overview of the disease and for PET scan you need an ameloid PET and a tau PET
but then you still don’t know anything about neurodegeneration
Lumbar is still invasive
3
, LUMBAR PUNCTURE (LP): guidelines
Has a lot of side effect but these were related to the needle so there are guidelines to minimize the side effects
AD DIAGNOSIS: CSF BIOMARKERS VS AMYLOID PET
CSF BIOMARKERS
Requires LP
• Relatively invasive
• Well-tolerated with minimal side effects
Analysis of AD CSF biomarkers
• Relatively cheap
• Overview AD pathology
High diagnostic yield: routine clinical practice for AD diagnosis
4
LES 1: Alzheimer’s and dementia from clinical perspective
(Engelborghs)
Dementia and Alzheimer's disease (AD): epidemiology
Since 2023: dementia = 1st cause of death in Belgium
develops dementia
As age is main risk factor and given ageing population, number of people with dementia is expected to have doubled in
2070
DEMENTIA = UMBRELLA
memory problems, spatial problems, .... are the symptoms but is not
the disease
people with dementia has 3 pilars
* cognitive pilar
* change of personality and behaviour
* functional deficits (activities of daily living become complex,
become dependent on others to survive)
if you think of dementia you think of memory problems and for AD
this is true this is the most common symptom but for FTLD the most
common symptom is behavioural problem
ALZHEIMER’S DISEASE (AD): THE AMYLOID CASCADE HYPOTHESIS
1) The formation of ameloid
plaques is the first thing that happens
in the brain
ameloid precursor protein produces
42 AZ ameloid beta protein which is
insoluble and then it starts clitting
together forming deposits in the brain
= ameloid plaques
Has a dense ameloid nucleus
In between the neurons
2) tau protein is the basis of the
cytoskeleton of neurons (for
structural reasons but also for
transport of neurotransmitters)
tau gets hyperphosphorylated and tau loses its function and forms aggregates and deposits of hyperphosphorylated tau =
neurofibrillary tangles
Within the neurons
3) Degeneration of neurons + number of synapses start decreasing (=synaptic degeneration)
This correlates with the cognitive decline in neurons
4) Loss of neurons themselves and schrinkage of the brain
Brain schrinkage is normal in aging but in AD it starts earlier and is more progressive
hippocampus is a structure that is important to transfer info to your memory
atrofie is max in hippocampus -> biomarker for diagnostic + recent memory problems
loss of neurons themselves and the brain schrinks = atrofie
1
,sequence of spread of neurofibrillary tangles
the darker the red, the higher the intensity of neurofibrillary
tangles
ameloid plaque are more localised so this doens't affect the
whole brain as compaired to this
MCI: people with for eg memory problems but for the rest are
normal because they don't have symptoms in the 3 pilars of
dementia
do all people with AD have dementia? NO, the first ameloid
plaques occure 20 years before the symptoms so brain 1 has
AD but no dementia
The Alzheimer continuum
you spend the majority of the disease in the preclinical stage
→ building up the disease without showing symptoms
The first diagnosis is the mild cognitive impairment -> new
methods are focused on diagnosis early dementia or MCI and
treating this
How is AD diagnosed?
make use of markers of the disease → coloured curves
are different markers we use in clinical practice
they move from normal to abnormal throughout the
different stages of the disease
ADL = activities of daily living
Functional deficits
MCI have no deficits but everyone with dementia
has deficits in ADL → every consultation of
someone with MCI we ask about deficits in ADL
and once there are deficits the person has
developed dementia
Neuropsychologists takes the history of patient & family to detect other causes of cognitive problems -> sleep problems
can also cause memory problems (is a complete other cause than dementia). Then he starts testing the different cognitive
functions to cover all cognitive domains → you have norms for these domains (“the mean score for this patient must be
X”)
Result of such test is “the cognitive function are normal for this age” or “has MCI” or he can specify for a specific domain
like everything is good but memory is affected -> can give a disease stage
Cornerstone of the diagnosis of dementia and AD. Can’t diagnose it without this
Biomarkers alone can give an incorrect diagnosis. Neuropsychologic exam should always be performed -> time consuming
and expensive
NEUROPSYCHOLOGICAL EXAMINATION
Requires neuropsychologist
Time-consuming: 2h of testing, 1h of data analysis and writing report Reimbursed once in a life-time for about half of the
cost price
Only AD biomarker testing if objective cognitive deficits in a consented patients (right to know versus right to refuse
diagnosis of an incurable disease)
2
,Thus:
1. Neuropsychology = required!
2. Neuropsychology = bottle neck in diagnostic work-up given number of neuropsychologists and reimbursement
MRI IN AD: HIPPOCAMPAL ATROPHY (blue curve)
Hippocampus is a small 3D structure that can be hard in the early
stages of the disease to diagnose the atrofie → that’s why we
nowadays use AI
develop AI based software pipeline and help with the analysis of
MR images for brain diseases
now incorporated in routine → after 30 min you get a report with
the brain volume in total, volumes of different parts of the brain
and the comparison with what is normal for that age
helps to detect hippocampal degeneration in earliest stages
CSF BIOMARKERS
red: ameloid curve = the first thing that happens in the brain
Ameloid PET to look at the ameloid deposits in the brain →
expensive (depending on the tracer + health care doesn’t pay
in Belgium) + capacity of PET scans is limited
Not used in clinical practice
Instead we do a lumbar puncture to withdraw CSF that finds
its origin in the brain so the metabolism of the brain is
reflected in the CSF → proteins linked to AD can be found
Ameloid beta of 42 az (main constituent of ameloid
plaques) → levels in the brain get lower in case of AD
Phosphorylated tau (main component of neurofibrillary
tangles) → increased in AD
Total tau fraction (composed of normal and
hyperphosphorylated tau) → increases in AD because
of neurodegeneration
Lumbar puncture is only to help diagnose and cannot help you with the severity of the disease → neuropsychological
exam gives severity
So one lumbar puncture gives the whole overview of the disease and for PET scan you need an ameloid PET and a tau PET
but then you still don’t know anything about neurodegeneration
Lumbar is still invasive
3
, LUMBAR PUNCTURE (LP): guidelines
Has a lot of side effect but these were related to the needle so there are guidelines to minimize the side effects
AD DIAGNOSIS: CSF BIOMARKERS VS AMYLOID PET
CSF BIOMARKERS
Requires LP
• Relatively invasive
• Well-tolerated with minimal side effects
Analysis of AD CSF biomarkers
• Relatively cheap
• Overview AD pathology
High diagnostic yield: routine clinical practice for AD diagnosis
4