, Inhoudsopgave
TASK 1: ANXIETY AND HYPERVENTILATION .................................................................................................. 4
HOW DOES STRESS WORK.............................................................................................................................. 4
WHAT IS ANXIETY ........................................................................................................................................... 7
SEVERAL PERSPECTIVES.................................................................................................................................. 8
ANXIETY DISORDERS (SYBTYPES, SYMPTOMS, COMORBIDITY, PREVALENCE..)......................................... 10
WHAT IS HYPERVENTILATION SYNDROME? ................................................................................................ 18
PHYSIOLOGICAL AND PSYCHOLOGICAL SIDE OF HYPERVENTILATION ........................................................ 18
COGNITIVE MODEL OF PANIC....................................................................................................................... 19
HYPERVENTILATION VS PANIC DISORDERS.................................................................................................. 19
TASK 2: FEAR AND PHOBIAS ...................................................................................................................... 20
WHAT IS A SPECIFIC PHOBIA (SUBTYPES, COMORBIDITY, DSM-5…)........................................................... 20
DEVELOPMENT OF A SPECIFIC PHOBIA (PATHWAYS OF FEAR) ................................................................... 22
HOW TO TREAT SPECIFIC PHOBIAS? ............................................................................................................ 22
MECHANISMS OF CHANGE ........................................................................................................................... 24
CRITISISM OF CONDITIONING AS EXPLANATION OF PHOBIAS ................................................................... 25
WHAT IS THE LEARNING THEORY ................................................................................................................. 26
COLLEGE: LEARNING THEORY .................................................................................................................... 30
ACQUISITION OF FEAR .................................................................................................................................. 30
GENERALIZATION OF FEAR ........................................................................................................................... 31
AVOIDANCE OF FEAR .................................................................................................................................... 31
EXTINCION .................................................................................................................................................... 33
TREATMENT .................................................................................................................................................. 34
SHORT SUMMARY ........................................................................................................................................ 34
TASK 3: IMPROVING EXPOSURE ................................................................................................................. 35
WHAT IS THE COGNITIVE THEORY? .............................................................................................................. 35
WHAT IS THE INFORMATION PROCESSING THEORY? .................................................................................. 38
COGNITIVE TREATMENTS ............................................................................................................................. 43
HOW DOES SAFETY BEHAVIOUR WORK?..................................................................................................... 45
CRITICAL READING ASSIGNMENT ................................................................................................................ 47
WHAT WOULD YOU ADVISE SASKIA TO DO? ............................................................................................... 47
COGNITIVE TRAINING COLLEGE ................................................................................................................... 48
COLLEGE: BRAIN AND NEUROIMAGING ..................................................................................................... 50
BRAIN FUNCTION AND HOW TO MEASURE ................................................................................................ 50
NEUROIMAGING IN ANXIETY DISORDERS ................................................................................................... 51
FEAR NETWORK ............................................................................................................................................ 53
DIFFERENT ANXIETY DISORDERS ................................................................................................................. 55
EXTINCTION AND EMOTION REGULATION .................................................................................................. 56
TREATMENT .................................................................................................................................................. 59
TASK 4: BIOLOGICAL SUBSTRACT OF PANIC & FEAR .................................................................................... 60
WHAT PATHWAYS ARE INVOLVED IN ANXIETY?........................................................................................... 60
WHAT NEUROTRANSMITTERS ARE INVOLVED IN ANXIETY? ....................................................................... 63
WHAT MEDICATION IS USED FOR ANXIETY? ............................................................................................... 66
....................................................................................................................................................................... 69
WHAT ARE THE BRAIN MECHANISMS THAT UNDERLIE THE EFFECTS OF TREATMENT? ............................ 70
2
,TASK 5: OCD and THOUGHT SUPRESSION ................................................................................................... 73
WHAT IS OCD? (PREVALENCE, COMORBIDITY, DIFFERENTIAL DIAGNOSIS) ............................................... 73
WHAT ARE THE SUBTYPES OF OCD? ............................................................................................................ 75
HOW CAN YOU TREAT OCD? ........................................................................................................................ 76
OBSESSIONS VS NORMAL WORRY ............................................................................................................... 76
WHAT ARE NORMAL AND ABNORMAL OBSESSIONS/COMPULSIONS? ..................................................... 78
HOW DO YOU DISTINGUISH OCD FROM OTHER DISORDERS? ................................................................... 79
WHAT IS THOUGHT SUPRESSION AND HOW DOES IT MAINTAIN OCD? .................................................... 79
WHAT IS THE ROLE OF CATASTROPHIC MISINTERPRETATION IN OCD? ...................................................... 82
WHY SHOULDN’T OCD BE CONSIDERED AN ANXIETY DISORDER? ............................................................. 83
BOB ............................................................................................................................................................... 83
TAAK 6: PTSD ............................................................................................................................................ 84
WHAT IS PTSD? ............................................................................................................................................. 84
THE RISK FACTORS OF PTSD ......................................................................................................................... 89
WHAT IS FRAGMENTED MEMORY, HOW DOES IT MAINTAIN PTSD?.......................................................... 90
TREATMENTS FOR PTSD ............................................................................................................................... 91
THEORETICAL PERSPECTIVES ON TRAUMA ................................................................................................. 93
TRAUMA IN ADULTHOOD VS CHILDHOOD .................................................................................................. 95
WHY IS PTSD NO LONGER CLASSIFIED AS AN ANXIETY DISORDER?........................................................... 95
TENTAMEN POTENTIE ............................................................................................................................... 96
TAAK 1 ........................................................................................................................................................... 96
TAAK 2 ........................................................................................................................................................... 98
TAAK 3 ........................................................................................................................................................... 99
TAAK 4 ......................................................................................................................................................... 100
TAAK 6 ......................................................................................................................................................... 101
3
, TASK 1: ANXIETY AND HYPERVENTILATION
HOW DOES STRESS WORK
Stress = the negative emotional and psychological process that occurs as individuals try to
adjust to or deal with stressors.
Stressors = are events and situations (such as exams or accidents) that disrupt or threaten to
disrupt a person’s daily functioning and sense of well-being.
Stress-reactions = the physical, psychological, and behavioral responses that occur in the
face of stressors (such as nausea, anxiety or avoidance).
Everyone gets affected by stress differently, there are several mediating factors that influence
this. These mediating effects are: the extent to which we can predict and control our
stressor; how we interpret the threat involved; the social support we get; and our skills for
coping with stress. So, stress is not a specific event but a transaction between people and
their environment.
Any event that forces a person to change or adapt can be a psychological stressor. Even nice
experiences can be stressful. For example, a wedding is supposed to be very nice, but it can
be really exhausting. But, situations that are unpleasant and difficult to cope with usually
produce the most negative psychological and physical effects. Think about catastrophic
events (like terrorism, explosions, hurricanes, plane crash), life changes or chronic stressors.
• Catastrophic events: are sudden, unexpected, potentially life-threatening
experiences or traumas. Physical or sexual assault, military combat, natural disasters,
terrorist attacks… fall into this category.
• Life changes and strains: include divorce, illness in the family, difficulties at work,
moving.. and other situations that demands people to adjust.
• Chronic stressors: they continue over a long period of time, think about terrorism,
having a serious illness, being unable to earn money, being a discrimination victim,
academic pressure for years..
• Daily hassles: think about irritations, pressures, and annoyances that may not be
major stressors by themselves but whose effects add up to become significant. Think
about heavy traffic that causes road rage.
Holmes and Rahe created the SRRS, Social Readjustment Rating Scale, calculates stressscore.
→ Maar deze scale heeft best wat kritiek, want hij kijkt namelijk vooral naar de stress die life
changing dingen veroorzaken. Zoals scheiden of je werk verliezen. Maar die life changes zijn
natuurlijk maar 1 onderdeel van het totale stress process, dus er werden wat uitgebreidere
schalen gemaakt. Hierin werd bijv coping, en mensen hun perceptie meegenomen.
4
, Physical responses
Immediate physical stress responses: rapid breathing,
increased heartbeat and blood pressure, sweating… →
This is part of the fight-or-flight system, this prepares
the body to be prepared to face or to flee an
immediate threat. En als de threat dan weg is dan
hoort die fight-flight reactie af te nemen, maar wat
nou als de threat niet afneemt?...
Long-term stressors: fight-or flight reactions are the
beginning of a longer series of physical/psychological
reactions: physical reactions to stress occur in a
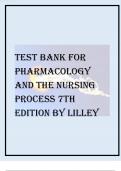
consistent pattern = Selye's model of general adaptation syndrome (GAS). It has 3 stages:
1) Alarm reaction: a version of the fight-or-flight reaction. This is a reaction to a mild
stressor, think a fitting room in the Zara that is way too hot, you start sweating to help
your body regulate the temperature.
• Alarm reactions are controlled by the
sympathetic nervous system via the
sympatho-adreno-medullary system, SAM:
Stressor → triggers a process in the brains
hypothalamus → The hypothalamus then
activates the autonomic nervous system
(ANS) → this then stimulates the medulla
(inner part) of the adrenal glands → then, the
adrenals secrete catecholamines (adrenaline
and noradrenaline) → this then affects
several organs (liver, hearth, lungs…) → this
action causes increased blood pressure,
muscle tention, blood sugar, and pupil size.
• Stressors also activate the HPA-system,
Hypothalamic-pituitary-adrenocortical:
hypothalamus stimulates the pituitary gland
in the brain → this then secretes hormones like ACTH (adrenocorticotropic
hormone) → ACTH stimulates the cortex (outer surface) of the adrenal glands →
the adrenal glands then secrete corticosteroids like cortisol → this hormone
releases the body’s energy supplies and fights excessive inflammation.
• These 2 stress systems, SAM en HPA, generate the energy that may be needed in
an emergency. In the stressor is persistant, the second stage starts.
2) Resistance stage: clear signs of the initial alarm reaction have faded. The drain on
adaptive energy is less during this stage, but the body is still working hard to cope
with stress. This state slowly but surely uses up the body’s reserves of adaptive
resources. As this happens, the body enters the 3 stage…
3) Exhaustion stage: this stage brings signs of physical wear and tear. Especially the
organs that were weak to begin with or that were heavily used in the resistant stage.
For example, if adrenaline and cortisol remain high for a long time, the result can be
damage to the heart and blood vessels; suppression of immune system; vulnerability
to illnesses like hearth disease, high blood pressure, artritis, colds and flu.
→ Ilnesses caused by stressors = diseases of adaptation.
5
,We have a parasympathetic up and down system.
1) Sympathetic (up): It causes our blood pressure, heartrate, respiration, sweating, and
blood in our muscles to increase. Goosebumps, your pupils get bigger… This all is so
that you are ready to take some action.
2) Parasympathetic (down): contraction of the bladder and intestinal (urge to go to the
toilet), digestion stops, sick feeling. Om dus op deze gebieden energie te besparen.
Psychological response
Selye’s GAS model has been very influential, maar heeft ook wel wat kritiek gekregen → For
underestimating the role of psychological facotres in stress. This led to the development of
psychobiological models = deze benadrukken the importance of psychological as well as
biological variables in regulating and producing stress responses. Deze psychological
responses to stress can appear as changes in….
• Emotional changes: de fysieke stress die je voelt gaat vaak gepaard met verandering
in je emoties. Als iemand een geweer in je nek zet, zal je hartslag zekerste weten
omhoog gaan, maar je zal ook een hele sterke angst emotie voelen. Vaak nemen die
emotie changes na een tijdje wel weer af, maar als dat niet gebeurt dan kunnen
mensen dus gediagnostiseerd worden met een GAD, MDD of andere disorder.
• Cognitive changes: typische cognitieve stressreacties zijn bijv niet goed kunnen
concentreren, niet logisch kunnen nadenken of slecht kunnen onthouden. Dit komt
soms door ruminative thinking = the repeated intrusion of thoughts about stressful
events. Een begrip wat hier ook van toepassing is is catastrophizing = dwelling on and
overemphasizing the potential consequences of negative events. Deze 2 dingen
belemmeren het cognitieve functioneren, waardoor iemand misschien nog een
sterkere stress response krijgt en nog meer anxiety. Hierdoor kun je ook weer
narrowing of attention krijgen waardoor je dus minder goed kan gaan problemsolven.
• Behavioral changes: denk hierbij aan gespannen gezichtsuitdrukkingen, een
bibberstem, tremors or spasms. Maar denk hierbij ook aan hoe mensen omgaan met
de stressor, door bijvoorbeeld vermijding. Denk aan aan de alcohol schieten,
overeten, veel slapen, agressief gedrag of zelfs zelfmoord plegen.
Wanneer is een stressor stressvoller?
Unpredictable stressors blijken meer impact te hebben dan wel voorspelbare stressors. Denk
bijv aan opa, oma heeft zich hier wel een jaar op kunnen voorbereiden, de klap van deze
stressor is dus minder groot dan dat het ineens was gebeurd. Ook de perception of control
heeft een mediating effect op de stressor. Als mensen het gevoel hebben controle te hebben
over een situatie is de stressor iets minder grote impact. Mensen blijken ook minder last te
hebben van de stressor als ze goede coping resources hebben, zoals geld of tijd. Als je een
auto-ongeluk hebt scheelt het bijv een hoop als je genoeg geld hebt om een nieuwe te
kopen. En ook als je effectieve coping methoden gebruikt kan dit helpen. Dit kan je zien in..
1) Problem focussed coping: dus bijv proberen de stressor te elimineren.
2) Emotion-focussed coping: reguleren van de negatieve emoties die erbij komen kijken
6
, WHAT IS ANXIETY
Anxiety = the feeling of fear or panic. Most people feel anxious, panicky or fearful about
situations in life, such as money problems or exams but often once this situation is over, you
feel better and calmer. Sometimes… this feeling of fear or anxiety continues after the difficult
situation or you may feel a stronger sense of fear than other people and this is when anxiety
might become a problem and can affect your daily life/functioning.
Fear: Anxiety:
• Threat present • Threat expected
• Clear threat source • No actual treat source
• Short • Long, can go on forever
• High tension • Discomfort
• Clear start • Unclear start
• Emergency/quick response • Heightened vigilance, your body is
always on and ready for danger.
Artikel Elevated Sympathetic Activity (Holden & Barlow, 1986)
• De onderzoekers zeggen eigenlijk ‘with anxious patients,
an anxiety-producing situation is not necessary to
produce hyperarousal; rather, it seems to be chronic.’ En
dit artikel ligt het toe met een experiment dat zij deden.
• Studie: Deelnemers: 10 vrouwen met paniekstoornis en
agorafobie + 10 controlepersonen (zonder
angststoornis), zorgvuldig gematcht. Taak: Deelnemers
liepen meerdere keren een wandelroute op een station
die steeds angstiger werd, terwijl hartslag en zelf-
gerapporteerde angst werden gemeten. Baselines: Er
werden ook rustmetingen gedaan: zittend in een stoel
(rust) en wandelend in het gebouw (zonder
angsttriggers).
• Belangrijkste bevindingen: Mensen met
paniekstoornis hadden bij álle wandelingen een
hogere hartslag dan de controlegroep. Het verschil
in hartslag kwam niet door de angstige taak zelf,
maar doordat de angstgroep ook in rust al een
verhoogde hartslag had = chronic overarousal.
Want als je de rust-hartslag aftrekt van de hartslag
tijdens de wandeling, was er géén verschil tussen
de groepen. Dit wijst erop dat de verhoogde
hartslag niet specifiek het gevolg was van de
angstige situatie, maar van een chronische staat
van verhoogde alertheid.
Resultaten van andere studies die dit beamen:
1) EEG-onderzoeken laten zien dat angstige mensen minder alfa-activiteit (gerelateerd
aan ontspanning) en meer bèta-activiteit (gerelateerd aan alertheid/spanning)
hebben. Harmonic driving: was much higher in anxious patients than in nonanxious
controls or depressed patients. Harmonic driving is een reactie van de hersenen
op knipperend licht, die reactie kan je zien op de EEG.
7
, 2) Results Lader & Wing: Na het aanbieden van 20 identieke luide geluiden (100 dB):
Alle controlegroep-deelnemers hadden volledig gehabitueerd (dus: geen GSR-
reacties meer). Slechts 6 van de angstige patiënten hadden volledig gehabitueerd.
Angstige patiënten vertoonden:
• Langzamere habituatie van de GSR (galvanic skin response).
• Meer spontane huidgeleidingsfluctuaties (meer "interne onrust").
• Gemiddeld 15 slagen per minuut hogere hartslag dan de controlegroep.
Er was een duidelijke relatie: → Hoe angstiger de patiënt werd beoordeeld,
hoe trager de habituatie en hoe meer spontane fysiologische reacties.
Normal patients and patients with specific phobias both quickly became habituated
and had fewer spontaneous skin fluctuations. Patients with specific phobias are not in
the same state of overarousal as other anxiety disorders. Nevertheless, the anxiety
states, as well as social phobia and agoraphobia, clearly show chronic
overstimulation.
Autonomic inflexibility: Bij mensen met een angststoornis is vaak sprake van autonome
inflexibiliteit. Dat betekent dat hun autonome zenuwstelsel – dat automatisch functies zoals
hartslag en ademhaling regelt – minder flexibel reageert op stressvolle of rustgevende
situaties. Vooral de parasympathische tak van het zenuwstelsel, die normaal zorgt voor
herstel en ontspanning, lijkt bij hen minder actief. Dit zie je terug in een lagere
hartslagvariabiliteit, wat betekent dat hun hartslag minder mee verandert met wat er in hun
omgeving gebeurt. Zelfs in rust is hun hartslag vaak constant hoog, terwijl bij gezonde
mensen de hartslag juist varieert. Onderzoek laat zien dat dit vooral samenhangt met
piekeren. Bij mensen met gegeneraliseerde angststoornis (GAS) is die lage variabiliteit zelfs in
rustige situaties aanwezig. Hun lichaam lijkt voortdurend in een soort paraatheidsstand te
staan, zonder voldoende herstel. Dit wordt gezien als een gevolg van chronisch negatieve
gedachten, en niet als iets dat enkel door een externe stressor wordt veroorzaakt. Het
lichaam past zich daardoor steeds minder goed aan aan verschillende situaties – een soort
verstarring in het zenuwstelsel. Deze autonome inflexibiliteit komt niet alleen voor bij GAS,
maar ook bij andere angststoornissen, zoals paniekstoornis en obsessief-compulsieve
stoornis. Zelfs bij angstige kinderen is een hogere rusthartslag en minder variatie daarin
waargenomen. Dit wijst erop dat het een breder kenmerk is van angststoornissen.
SEVERAL PERSPECTIVES
Social psychological view: Terror Management Theory
= the basic gist of the theory is that humans are motivated to cope with the potential for
terror inherent in the human awareness of vulnerability and mortality by investing in cultural
belief systems… since its inception, the theory has generated empirical research into not just
the nature of self-esteem motivation and prejudice, but also host of other forms of human
social behaviors… depression and psychopathology.
• Self-esteem: Self-esteem consists of the perception that one is a valuable member of
a meaningful universe. Je wilt dus het idee hebben dat je een valuable member bent
van de samenleving, want zo heeft je leven een betekenis.
• Anxiety: How does it develop? Usually when someone is 3 years old children begin to
learn about and become concerned with the problem of death and anxieties
regarding darkness and monsters become more and more linked to real treats … that
culminate with the realization of the inevitability of death.
8
TASK 1: ANXIETY AND HYPERVENTILATION .................................................................................................. 4
HOW DOES STRESS WORK.............................................................................................................................. 4
WHAT IS ANXIETY ........................................................................................................................................... 7
SEVERAL PERSPECTIVES.................................................................................................................................. 8
ANXIETY DISORDERS (SYBTYPES, SYMPTOMS, COMORBIDITY, PREVALENCE..)......................................... 10
WHAT IS HYPERVENTILATION SYNDROME? ................................................................................................ 18
PHYSIOLOGICAL AND PSYCHOLOGICAL SIDE OF HYPERVENTILATION ........................................................ 18
COGNITIVE MODEL OF PANIC....................................................................................................................... 19
HYPERVENTILATION VS PANIC DISORDERS.................................................................................................. 19
TASK 2: FEAR AND PHOBIAS ...................................................................................................................... 20
WHAT IS A SPECIFIC PHOBIA (SUBTYPES, COMORBIDITY, DSM-5…)........................................................... 20
DEVELOPMENT OF A SPECIFIC PHOBIA (PATHWAYS OF FEAR) ................................................................... 22
HOW TO TREAT SPECIFIC PHOBIAS? ............................................................................................................ 22
MECHANISMS OF CHANGE ........................................................................................................................... 24
CRITISISM OF CONDITIONING AS EXPLANATION OF PHOBIAS ................................................................... 25
WHAT IS THE LEARNING THEORY ................................................................................................................. 26
COLLEGE: LEARNING THEORY .................................................................................................................... 30
ACQUISITION OF FEAR .................................................................................................................................. 30
GENERALIZATION OF FEAR ........................................................................................................................... 31
AVOIDANCE OF FEAR .................................................................................................................................... 31
EXTINCION .................................................................................................................................................... 33
TREATMENT .................................................................................................................................................. 34
SHORT SUMMARY ........................................................................................................................................ 34
TASK 3: IMPROVING EXPOSURE ................................................................................................................. 35
WHAT IS THE COGNITIVE THEORY? .............................................................................................................. 35
WHAT IS THE INFORMATION PROCESSING THEORY? .................................................................................. 38
COGNITIVE TREATMENTS ............................................................................................................................. 43
HOW DOES SAFETY BEHAVIOUR WORK?..................................................................................................... 45
CRITICAL READING ASSIGNMENT ................................................................................................................ 47
WHAT WOULD YOU ADVISE SASKIA TO DO? ............................................................................................... 47
COGNITIVE TRAINING COLLEGE ................................................................................................................... 48
COLLEGE: BRAIN AND NEUROIMAGING ..................................................................................................... 50
BRAIN FUNCTION AND HOW TO MEASURE ................................................................................................ 50
NEUROIMAGING IN ANXIETY DISORDERS ................................................................................................... 51
FEAR NETWORK ............................................................................................................................................ 53
DIFFERENT ANXIETY DISORDERS ................................................................................................................. 55
EXTINCTION AND EMOTION REGULATION .................................................................................................. 56
TREATMENT .................................................................................................................................................. 59
TASK 4: BIOLOGICAL SUBSTRACT OF PANIC & FEAR .................................................................................... 60
WHAT PATHWAYS ARE INVOLVED IN ANXIETY?........................................................................................... 60
WHAT NEUROTRANSMITTERS ARE INVOLVED IN ANXIETY? ....................................................................... 63
WHAT MEDICATION IS USED FOR ANXIETY? ............................................................................................... 66
....................................................................................................................................................................... 69
WHAT ARE THE BRAIN MECHANISMS THAT UNDERLIE THE EFFECTS OF TREATMENT? ............................ 70
2
,TASK 5: OCD and THOUGHT SUPRESSION ................................................................................................... 73
WHAT IS OCD? (PREVALENCE, COMORBIDITY, DIFFERENTIAL DIAGNOSIS) ............................................... 73
WHAT ARE THE SUBTYPES OF OCD? ............................................................................................................ 75
HOW CAN YOU TREAT OCD? ........................................................................................................................ 76
OBSESSIONS VS NORMAL WORRY ............................................................................................................... 76
WHAT ARE NORMAL AND ABNORMAL OBSESSIONS/COMPULSIONS? ..................................................... 78
HOW DO YOU DISTINGUISH OCD FROM OTHER DISORDERS? ................................................................... 79
WHAT IS THOUGHT SUPRESSION AND HOW DOES IT MAINTAIN OCD? .................................................... 79
WHAT IS THE ROLE OF CATASTROPHIC MISINTERPRETATION IN OCD? ...................................................... 82
WHY SHOULDN’T OCD BE CONSIDERED AN ANXIETY DISORDER? ............................................................. 83
BOB ............................................................................................................................................................... 83
TAAK 6: PTSD ............................................................................................................................................ 84
WHAT IS PTSD? ............................................................................................................................................. 84
THE RISK FACTORS OF PTSD ......................................................................................................................... 89
WHAT IS FRAGMENTED MEMORY, HOW DOES IT MAINTAIN PTSD?.......................................................... 90
TREATMENTS FOR PTSD ............................................................................................................................... 91
THEORETICAL PERSPECTIVES ON TRAUMA ................................................................................................. 93
TRAUMA IN ADULTHOOD VS CHILDHOOD .................................................................................................. 95
WHY IS PTSD NO LONGER CLASSIFIED AS AN ANXIETY DISORDER?........................................................... 95
TENTAMEN POTENTIE ............................................................................................................................... 96
TAAK 1 ........................................................................................................................................................... 96
TAAK 2 ........................................................................................................................................................... 98
TAAK 3 ........................................................................................................................................................... 99
TAAK 4 ......................................................................................................................................................... 100
TAAK 6 ......................................................................................................................................................... 101
3
, TASK 1: ANXIETY AND HYPERVENTILATION
HOW DOES STRESS WORK
Stress = the negative emotional and psychological process that occurs as individuals try to
adjust to or deal with stressors.
Stressors = are events and situations (such as exams or accidents) that disrupt or threaten to
disrupt a person’s daily functioning and sense of well-being.
Stress-reactions = the physical, psychological, and behavioral responses that occur in the
face of stressors (such as nausea, anxiety or avoidance).
Everyone gets affected by stress differently, there are several mediating factors that influence
this. These mediating effects are: the extent to which we can predict and control our
stressor; how we interpret the threat involved; the social support we get; and our skills for
coping with stress. So, stress is not a specific event but a transaction between people and
their environment.
Any event that forces a person to change or adapt can be a psychological stressor. Even nice
experiences can be stressful. For example, a wedding is supposed to be very nice, but it can
be really exhausting. But, situations that are unpleasant and difficult to cope with usually
produce the most negative psychological and physical effects. Think about catastrophic
events (like terrorism, explosions, hurricanes, plane crash), life changes or chronic stressors.
• Catastrophic events: are sudden, unexpected, potentially life-threatening
experiences or traumas. Physical or sexual assault, military combat, natural disasters,
terrorist attacks… fall into this category.
• Life changes and strains: include divorce, illness in the family, difficulties at work,
moving.. and other situations that demands people to adjust.
• Chronic stressors: they continue over a long period of time, think about terrorism,
having a serious illness, being unable to earn money, being a discrimination victim,
academic pressure for years..
• Daily hassles: think about irritations, pressures, and annoyances that may not be
major stressors by themselves but whose effects add up to become significant. Think
about heavy traffic that causes road rage.
Holmes and Rahe created the SRRS, Social Readjustment Rating Scale, calculates stressscore.
→ Maar deze scale heeft best wat kritiek, want hij kijkt namelijk vooral naar de stress die life
changing dingen veroorzaken. Zoals scheiden of je werk verliezen. Maar die life changes zijn
natuurlijk maar 1 onderdeel van het totale stress process, dus er werden wat uitgebreidere
schalen gemaakt. Hierin werd bijv coping, en mensen hun perceptie meegenomen.
4
, Physical responses
Immediate physical stress responses: rapid breathing,
increased heartbeat and blood pressure, sweating… →
This is part of the fight-or-flight system, this prepares
the body to be prepared to face or to flee an
immediate threat. En als de threat dan weg is dan
hoort die fight-flight reactie af te nemen, maar wat
nou als de threat niet afneemt?...
Long-term stressors: fight-or flight reactions are the
beginning of a longer series of physical/psychological
reactions: physical reactions to stress occur in a
consistent pattern = Selye's model of general adaptation syndrome (GAS). It has 3 stages:
1) Alarm reaction: a version of the fight-or-flight reaction. This is a reaction to a mild
stressor, think a fitting room in the Zara that is way too hot, you start sweating to help
your body regulate the temperature.
• Alarm reactions are controlled by the
sympathetic nervous system via the
sympatho-adreno-medullary system, SAM:
Stressor → triggers a process in the brains
hypothalamus → The hypothalamus then
activates the autonomic nervous system
(ANS) → this then stimulates the medulla
(inner part) of the adrenal glands → then, the
adrenals secrete catecholamines (adrenaline
and noradrenaline) → this then affects
several organs (liver, hearth, lungs…) → this
action causes increased blood pressure,
muscle tention, blood sugar, and pupil size.
• Stressors also activate the HPA-system,
Hypothalamic-pituitary-adrenocortical:
hypothalamus stimulates the pituitary gland
in the brain → this then secretes hormones like ACTH (adrenocorticotropic
hormone) → ACTH stimulates the cortex (outer surface) of the adrenal glands →
the adrenal glands then secrete corticosteroids like cortisol → this hormone
releases the body’s energy supplies and fights excessive inflammation.
• These 2 stress systems, SAM en HPA, generate the energy that may be needed in
an emergency. In the stressor is persistant, the second stage starts.
2) Resistance stage: clear signs of the initial alarm reaction have faded. The drain on
adaptive energy is less during this stage, but the body is still working hard to cope
with stress. This state slowly but surely uses up the body’s reserves of adaptive
resources. As this happens, the body enters the 3 stage…
3) Exhaustion stage: this stage brings signs of physical wear and tear. Especially the
organs that were weak to begin with or that were heavily used in the resistant stage.
For example, if adrenaline and cortisol remain high for a long time, the result can be
damage to the heart and blood vessels; suppression of immune system; vulnerability
to illnesses like hearth disease, high blood pressure, artritis, colds and flu.
→ Ilnesses caused by stressors = diseases of adaptation.
5
,We have a parasympathetic up and down system.
1) Sympathetic (up): It causes our blood pressure, heartrate, respiration, sweating, and
blood in our muscles to increase. Goosebumps, your pupils get bigger… This all is so
that you are ready to take some action.
2) Parasympathetic (down): contraction of the bladder and intestinal (urge to go to the
toilet), digestion stops, sick feeling. Om dus op deze gebieden energie te besparen.
Psychological response
Selye’s GAS model has been very influential, maar heeft ook wel wat kritiek gekregen → For
underestimating the role of psychological facotres in stress. This led to the development of
psychobiological models = deze benadrukken the importance of psychological as well as
biological variables in regulating and producing stress responses. Deze psychological
responses to stress can appear as changes in….
• Emotional changes: de fysieke stress die je voelt gaat vaak gepaard met verandering
in je emoties. Als iemand een geweer in je nek zet, zal je hartslag zekerste weten
omhoog gaan, maar je zal ook een hele sterke angst emotie voelen. Vaak nemen die
emotie changes na een tijdje wel weer af, maar als dat niet gebeurt dan kunnen
mensen dus gediagnostiseerd worden met een GAD, MDD of andere disorder.
• Cognitive changes: typische cognitieve stressreacties zijn bijv niet goed kunnen
concentreren, niet logisch kunnen nadenken of slecht kunnen onthouden. Dit komt
soms door ruminative thinking = the repeated intrusion of thoughts about stressful
events. Een begrip wat hier ook van toepassing is is catastrophizing = dwelling on and
overemphasizing the potential consequences of negative events. Deze 2 dingen
belemmeren het cognitieve functioneren, waardoor iemand misschien nog een
sterkere stress response krijgt en nog meer anxiety. Hierdoor kun je ook weer
narrowing of attention krijgen waardoor je dus minder goed kan gaan problemsolven.
• Behavioral changes: denk hierbij aan gespannen gezichtsuitdrukkingen, een
bibberstem, tremors or spasms. Maar denk hierbij ook aan hoe mensen omgaan met
de stressor, door bijvoorbeeld vermijding. Denk aan aan de alcohol schieten,
overeten, veel slapen, agressief gedrag of zelfs zelfmoord plegen.
Wanneer is een stressor stressvoller?
Unpredictable stressors blijken meer impact te hebben dan wel voorspelbare stressors. Denk
bijv aan opa, oma heeft zich hier wel een jaar op kunnen voorbereiden, de klap van deze
stressor is dus minder groot dan dat het ineens was gebeurd. Ook de perception of control
heeft een mediating effect op de stressor. Als mensen het gevoel hebben controle te hebben
over een situatie is de stressor iets minder grote impact. Mensen blijken ook minder last te
hebben van de stressor als ze goede coping resources hebben, zoals geld of tijd. Als je een
auto-ongeluk hebt scheelt het bijv een hoop als je genoeg geld hebt om een nieuwe te
kopen. En ook als je effectieve coping methoden gebruikt kan dit helpen. Dit kan je zien in..
1) Problem focussed coping: dus bijv proberen de stressor te elimineren.
2) Emotion-focussed coping: reguleren van de negatieve emoties die erbij komen kijken
6
, WHAT IS ANXIETY
Anxiety = the feeling of fear or panic. Most people feel anxious, panicky or fearful about
situations in life, such as money problems or exams but often once this situation is over, you
feel better and calmer. Sometimes… this feeling of fear or anxiety continues after the difficult
situation or you may feel a stronger sense of fear than other people and this is when anxiety
might become a problem and can affect your daily life/functioning.
Fear: Anxiety:
• Threat present • Threat expected
• Clear threat source • No actual treat source
• Short • Long, can go on forever
• High tension • Discomfort
• Clear start • Unclear start
• Emergency/quick response • Heightened vigilance, your body is
always on and ready for danger.
Artikel Elevated Sympathetic Activity (Holden & Barlow, 1986)
• De onderzoekers zeggen eigenlijk ‘with anxious patients,
an anxiety-producing situation is not necessary to
produce hyperarousal; rather, it seems to be chronic.’ En
dit artikel ligt het toe met een experiment dat zij deden.
• Studie: Deelnemers: 10 vrouwen met paniekstoornis en
agorafobie + 10 controlepersonen (zonder
angststoornis), zorgvuldig gematcht. Taak: Deelnemers
liepen meerdere keren een wandelroute op een station
die steeds angstiger werd, terwijl hartslag en zelf-
gerapporteerde angst werden gemeten. Baselines: Er
werden ook rustmetingen gedaan: zittend in een stoel
(rust) en wandelend in het gebouw (zonder
angsttriggers).
• Belangrijkste bevindingen: Mensen met
paniekstoornis hadden bij álle wandelingen een
hogere hartslag dan de controlegroep. Het verschil
in hartslag kwam niet door de angstige taak zelf,
maar doordat de angstgroep ook in rust al een
verhoogde hartslag had = chronic overarousal.
Want als je de rust-hartslag aftrekt van de hartslag
tijdens de wandeling, was er géén verschil tussen
de groepen. Dit wijst erop dat de verhoogde
hartslag niet specifiek het gevolg was van de
angstige situatie, maar van een chronische staat
van verhoogde alertheid.
Resultaten van andere studies die dit beamen:
1) EEG-onderzoeken laten zien dat angstige mensen minder alfa-activiteit (gerelateerd
aan ontspanning) en meer bèta-activiteit (gerelateerd aan alertheid/spanning)
hebben. Harmonic driving: was much higher in anxious patients than in nonanxious
controls or depressed patients. Harmonic driving is een reactie van de hersenen
op knipperend licht, die reactie kan je zien op de EEG.
7
, 2) Results Lader & Wing: Na het aanbieden van 20 identieke luide geluiden (100 dB):
Alle controlegroep-deelnemers hadden volledig gehabitueerd (dus: geen GSR-
reacties meer). Slechts 6 van de angstige patiënten hadden volledig gehabitueerd.
Angstige patiënten vertoonden:
• Langzamere habituatie van de GSR (galvanic skin response).
• Meer spontane huidgeleidingsfluctuaties (meer "interne onrust").
• Gemiddeld 15 slagen per minuut hogere hartslag dan de controlegroep.
Er was een duidelijke relatie: → Hoe angstiger de patiënt werd beoordeeld,
hoe trager de habituatie en hoe meer spontane fysiologische reacties.
Normal patients and patients with specific phobias both quickly became habituated
and had fewer spontaneous skin fluctuations. Patients with specific phobias are not in
the same state of overarousal as other anxiety disorders. Nevertheless, the anxiety
states, as well as social phobia and agoraphobia, clearly show chronic
overstimulation.
Autonomic inflexibility: Bij mensen met een angststoornis is vaak sprake van autonome
inflexibiliteit. Dat betekent dat hun autonome zenuwstelsel – dat automatisch functies zoals
hartslag en ademhaling regelt – minder flexibel reageert op stressvolle of rustgevende
situaties. Vooral de parasympathische tak van het zenuwstelsel, die normaal zorgt voor
herstel en ontspanning, lijkt bij hen minder actief. Dit zie je terug in een lagere
hartslagvariabiliteit, wat betekent dat hun hartslag minder mee verandert met wat er in hun
omgeving gebeurt. Zelfs in rust is hun hartslag vaak constant hoog, terwijl bij gezonde
mensen de hartslag juist varieert. Onderzoek laat zien dat dit vooral samenhangt met
piekeren. Bij mensen met gegeneraliseerde angststoornis (GAS) is die lage variabiliteit zelfs in
rustige situaties aanwezig. Hun lichaam lijkt voortdurend in een soort paraatheidsstand te
staan, zonder voldoende herstel. Dit wordt gezien als een gevolg van chronisch negatieve
gedachten, en niet als iets dat enkel door een externe stressor wordt veroorzaakt. Het
lichaam past zich daardoor steeds minder goed aan aan verschillende situaties – een soort
verstarring in het zenuwstelsel. Deze autonome inflexibiliteit komt niet alleen voor bij GAS,
maar ook bij andere angststoornissen, zoals paniekstoornis en obsessief-compulsieve
stoornis. Zelfs bij angstige kinderen is een hogere rusthartslag en minder variatie daarin
waargenomen. Dit wijst erop dat het een breder kenmerk is van angststoornissen.
SEVERAL PERSPECTIVES
Social psychological view: Terror Management Theory
= the basic gist of the theory is that humans are motivated to cope with the potential for
terror inherent in the human awareness of vulnerability and mortality by investing in cultural
belief systems… since its inception, the theory has generated empirical research into not just
the nature of self-esteem motivation and prejudice, but also host of other forms of human
social behaviors… depression and psychopathology.
• Self-esteem: Self-esteem consists of the perception that one is a valuable member of
a meaningful universe. Je wilt dus het idee hebben dat je een valuable member bent
van de samenleving, want zo heeft je leven een betekenis.
• Anxiety: How does it develop? Usually when someone is 3 years old children begin to
learn about and become concerned with the problem of death and anxieties
regarding darkness and monsters become more and more linked to real treats … that
culminate with the realization of the inevitability of death.
8