Ortiz-Egea et al. J Med Case Reports (2021) 15:15
https://doi.org/10.1186/s13256-020-02620-5
Retinal imaging study
diagnoses in COVID-19: a
case report
Abstract
Background: Hyperreflective lesions at the level of ganglion cell (GCL) and inner plexiform
retinal layers (IPL) by optical coherence tomography (OCT) and cotton wool spots in the
examination of the eye fundus have recently been described as findings in patients with
COVID‑19 infection.
Case report: We report the case of a 42‑year‑old healthy Caucasian male anesthetist who
had treated COVID‑19 patients during the previous 5 weeks and suddenly presented with a
temporal relative scotoma in his left eye. Best‑ corrected visual acuity was 20/20 for the left
eye, and no discromatopsy or afferent pupillary defect was present.
Visual field test was performed, with no significant findings associated with the focal loss of
sensitivity described by the patient. The anterior segment was unremarkable on slit lamp
examination in both eyes. Fundus examination of the left eye showed no significant findings. A
placoid, hyperreflective band at the level of the GCL and IPL was visible in OCT which spared
the outer retina, at the time of diagnosis and 1 month later. An oropharyngeal swab test was
performed for severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) ribonucleic acid
(RNA), immunoglobulin G (IgG) and immunoglobulin M (IgM) enzyme‑linked immunosorbent
assay (ELISA) determination. Real‑time reverse‑ transcriptase polymerase chain reaction
(RT‑PCR) was negative. ELISA testing and a third rapid antibody detection test performed 7
days after the onset of symptoms were positive.
Conclusions: Ocular signs and symptoms in COVID‑19 cases are rarely reported, but may be
underestimated, espe‑ cially those that affect the retina and occur in asymptomatic or
paucisymptomatic cases. We present a case of COVID‑ 19 diagnosis based on retinal ophthalmic
examination.
Keywords: OCT, COVID‑19, SARS‑CoV‑2, Ophthalmology, Retina
Background
COVID-19 can cause pathological ophthalmologic
Coronavirus disease 2019 (COVID-19) is caused by
involvement, including conjunctivitis, chemosis, hyper-
severe acute respiratory syndrome coronavirus 2 (SARS-
emia, epiphora, secretion [2], photophobia, dry eye [3],
CoV-2). In humans, diseases of the coronavirus family
neuro-ophthalmic manifestations such as optic neuritis,
range from the mild common cold to more severe dis-
cranial nerve palsies, nystagmus or visual field defects
eases such as Middle East respiratory syndrome (MERS)
[4], and descriptions of retinal aggression [5, 6].
and SARS [1].
Optical coherence tomography (OCT) has proved to
be a useful tool for the in vivo study of the retina, where
hyperreflective structures range from normal retina
(nerve, fiber layer, inner and outer plexiform layers),
nerve fiber layer myelination or vessels, to lesions such as
hard exudates, haemorrhages, fibrosis, or focal inflamma-
tion, among others. Some of those imply the appearance
, of a shadow below said structures that may lead to
coagulopathy alterations. The patient had normal blood
inter- pretation errors [7].
pressure values.
After identifying the aforementioned retinal lesions
Case presentation
and considering the patient’s high-risk profession with
We present the case of a 42-year-old, healthy
regard to COVID-19 exposure, a pharyngeal swab test
Caucasian male anesthetist who had been working with
for SARS-CoV-2 ribonucleic acid (RNA) and enzyme-
COVID-19 patients during the 5 weeks prior to onset,
linked immunosorbent assay (ELISA) determination
who presented with a sudden temporal relative scotoma
of immunoglobulin G (IgG) and immunoglobulin M
in the left eye. The patient had no previous retinal
(IgM) were requested. At that time, the patient remem-
disease or systemic disease with retinal compromise.
bers that he had limited ageusia for several days 3
Best-corrected visual acuity was 20/20 for the left eye,
weeks before the onset of the scotoma. Real-time
and no discromatopsy or afferent pupillary defect was
reverse-tran- scriptase polymerase chain reaction (RT-PCR)
present. A visual field test (SITA Fast 30-2) was performed,
was nega- tive. ELISA testing and a third rapid antibody
with no significant find- ings associated with a focal loss
detection test performed 7 days after the onset of
of sensitivity described by the patient. The anterior
symptoms were positive.
segment and fundus exami- nation were unremarkable
In the subsequent follow-up of the patient 30 days
in both eyes.
after the start of the scotoma perception, he continued
Swept-source optical coherence tomography (SS-OCT,
to describe it. Retinal imaging study showed the same
Topcon Co., Tokyo, Japan) showed a hyperreflective band
hyperreflective lesions observed in SS-OCT, with even
at the level of ganglion cell and inner plexiform layers,
greater intensity (Fig. 2a, b), and there were no arteries or
which spared the outer retina (Fig. 1a, b). Multimodal
veins in the inner layers of the retina on this B-scan that
imaging showed neither hypo- nor hyper-autofluores-
could cause a hyperreflective shadow.
cence in the area. Fluorescein angiography showed no
areas of leakage or vascular exudation in early or late
Discussion and conclusions
phases.
Back in 2013, Sarraf et al. were the first to describe the
The patient did not report respiratory symptoms, fever
presence of multiple or isolated band-shaped, focal or
or any other clinical symptoms typically described in
diffuse hyperreflective lesions visible at the level of the
COVID-19 cases. Thoracic computed tomography imag-
internal nuclear layer in patients who presented with
ing did not show lesions compatible with those described
acute onset of a negative scotoma, which they called par-
in COVID-19 cases with respiratory involvement.
acentral acute medial maculopathy (PAMM). PAMM is a
Blood tests performed were normal, with no signs of
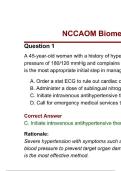
Fig. 1 a and b Swept‑source optical coherence
tomography (SS‑OCT, Topcon Co., Tokyo, Japan) showed
Fig. 2 a and b One month later, SS‑OCT follow‑up shows a
a hyperreflective band (yellow arrows) at the level of the
more prominent hyperreflective band at the level of
ganglion cell and inner plexiform retinal layers, which
ganglion cell and inner plexiform retinal layers (yellow
spared the outer retina. Green line where the B‑scan of
arrows). An en face infrared fundus image with a green
the OCT was acquired superposed automatically by the
line where the OCT B‑scan was acquired automatically
acquisition instrument on an en face infrared fundus
overlaid by the acquisition instrument. On the left, the
image, where there are signs of arterial and venous vessel
hyperreflective signal corresponds to the layer of nerve
reflexes (red asterisks) and nerve fiber layer
fibers (green star) and reflex vessels (red asterisks)
hyperreflectivity (green star)
https://doi.org/10.1186/s13256-020-02620-5
Retinal imaging study
diagnoses in COVID-19: a
case report
Abstract
Background: Hyperreflective lesions at the level of ganglion cell (GCL) and inner plexiform
retinal layers (IPL) by optical coherence tomography (OCT) and cotton wool spots in the
examination of the eye fundus have recently been described as findings in patients with
COVID‑19 infection.
Case report: We report the case of a 42‑year‑old healthy Caucasian male anesthetist who
had treated COVID‑19 patients during the previous 5 weeks and suddenly presented with a
temporal relative scotoma in his left eye. Best‑ corrected visual acuity was 20/20 for the left
eye, and no discromatopsy or afferent pupillary defect was present.
Visual field test was performed, with no significant findings associated with the focal loss of
sensitivity described by the patient. The anterior segment was unremarkable on slit lamp
examination in both eyes. Fundus examination of the left eye showed no significant findings. A
placoid, hyperreflective band at the level of the GCL and IPL was visible in OCT which spared
the outer retina, at the time of diagnosis and 1 month later. An oropharyngeal swab test was
performed for severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) ribonucleic acid
(RNA), immunoglobulin G (IgG) and immunoglobulin M (IgM) enzyme‑linked immunosorbent
assay (ELISA) determination. Real‑time reverse‑ transcriptase polymerase chain reaction
(RT‑PCR) was negative. ELISA testing and a third rapid antibody detection test performed 7
days after the onset of symptoms were positive.
Conclusions: Ocular signs and symptoms in COVID‑19 cases are rarely reported, but may be
underestimated, espe‑ cially those that affect the retina and occur in asymptomatic or
paucisymptomatic cases. We present a case of COVID‑ 19 diagnosis based on retinal ophthalmic
examination.
Keywords: OCT, COVID‑19, SARS‑CoV‑2, Ophthalmology, Retina
Background
COVID-19 can cause pathological ophthalmologic
Coronavirus disease 2019 (COVID-19) is caused by
involvement, including conjunctivitis, chemosis, hyper-
severe acute respiratory syndrome coronavirus 2 (SARS-
emia, epiphora, secretion [2], photophobia, dry eye [3],
CoV-2). In humans, diseases of the coronavirus family
neuro-ophthalmic manifestations such as optic neuritis,
range from the mild common cold to more severe dis-
cranial nerve palsies, nystagmus or visual field defects
eases such as Middle East respiratory syndrome (MERS)
[4], and descriptions of retinal aggression [5, 6].
and SARS [1].
Optical coherence tomography (OCT) has proved to
be a useful tool for the in vivo study of the retina, where
hyperreflective structures range from normal retina
(nerve, fiber layer, inner and outer plexiform layers),
nerve fiber layer myelination or vessels, to lesions such as
hard exudates, haemorrhages, fibrosis, or focal inflamma-
tion, among others. Some of those imply the appearance
, of a shadow below said structures that may lead to
coagulopathy alterations. The patient had normal blood
inter- pretation errors [7].
pressure values.
After identifying the aforementioned retinal lesions
Case presentation
and considering the patient’s high-risk profession with
We present the case of a 42-year-old, healthy
regard to COVID-19 exposure, a pharyngeal swab test
Caucasian male anesthetist who had been working with
for SARS-CoV-2 ribonucleic acid (RNA) and enzyme-
COVID-19 patients during the 5 weeks prior to onset,
linked immunosorbent assay (ELISA) determination
who presented with a sudden temporal relative scotoma
of immunoglobulin G (IgG) and immunoglobulin M
in the left eye. The patient had no previous retinal
(IgM) were requested. At that time, the patient remem-
disease or systemic disease with retinal compromise.
bers that he had limited ageusia for several days 3
Best-corrected visual acuity was 20/20 for the left eye,
weeks before the onset of the scotoma. Real-time
and no discromatopsy or afferent pupillary defect was
reverse-tran- scriptase polymerase chain reaction (RT-PCR)
present. A visual field test (SITA Fast 30-2) was performed,
was nega- tive. ELISA testing and a third rapid antibody
with no significant find- ings associated with a focal loss
detection test performed 7 days after the onset of
of sensitivity described by the patient. The anterior
symptoms were positive.
segment and fundus exami- nation were unremarkable
In the subsequent follow-up of the patient 30 days
in both eyes.
after the start of the scotoma perception, he continued
Swept-source optical coherence tomography (SS-OCT,
to describe it. Retinal imaging study showed the same
Topcon Co., Tokyo, Japan) showed a hyperreflective band
hyperreflective lesions observed in SS-OCT, with even
at the level of ganglion cell and inner plexiform layers,
greater intensity (Fig. 2a, b), and there were no arteries or
which spared the outer retina (Fig. 1a, b). Multimodal
veins in the inner layers of the retina on this B-scan that
imaging showed neither hypo- nor hyper-autofluores-
could cause a hyperreflective shadow.
cence in the area. Fluorescein angiography showed no
areas of leakage or vascular exudation in early or late
Discussion and conclusions
phases.
Back in 2013, Sarraf et al. were the first to describe the
The patient did not report respiratory symptoms, fever
presence of multiple or isolated band-shaped, focal or
or any other clinical symptoms typically described in
diffuse hyperreflective lesions visible at the level of the
COVID-19 cases. Thoracic computed tomography imag-
internal nuclear layer in patients who presented with
ing did not show lesions compatible with those described
acute onset of a negative scotoma, which they called par-
in COVID-19 cases with respiratory involvement.
acentral acute medial maculopathy (PAMM). PAMM is a
Blood tests performed were normal, with no signs of
Fig. 1 a and b Swept‑source optical coherence
tomography (SS‑OCT, Topcon Co., Tokyo, Japan) showed
Fig. 2 a and b One month later, SS‑OCT follow‑up shows a
a hyperreflective band (yellow arrows) at the level of the
more prominent hyperreflective band at the level of
ganglion cell and inner plexiform retinal layers, which
ganglion cell and inner plexiform retinal layers (yellow
spared the outer retina. Green line where the B‑scan of
arrows). An en face infrared fundus image with a green
the OCT was acquired superposed automatically by the
line where the OCT B‑scan was acquired automatically
acquisition instrument on an en face infrared fundus
overlaid by the acquisition instrument. On the left, the
image, where there are signs of arterial and venous vessel
hyperreflective signal corresponds to the layer of nerve
reflexes (red asterisks) and nerve fiber layer
fibers (green star) and reflex vessels (red asterisks)
hyperreflectivity (green star)