Affective Science and Psychopathology
lecture notes
Week 1: Introduction lecture
Learning objectives
1. Summarize in what form affect and its regulation might be disrupted in psychopathological
processes
2. Reflect on the recent state of affairs and possible improvements in psychological clinical practice
by use of affective science.
3. Argue how transdiagnostic models can contribute to understanding origin and maintenance of
psychopathology, yet also come with potential challenges
Affective processes
Affect = involves an evaluation of a situation as salient (belangrijk) and thereby triggering an
evolutionary adaptive response. Consist of:
Subjective (negative or positive feeling) components
Behavioral (motor expression or inclination (neiging)) components
Physiological (brain/body) components
Affective science
= the scientific study of affective processes. Affected processes is an umbrella term.
- Event-focus = to what extent is the affective process coupled with an event.
- Embodiment = how strong is the physical component.
Affective disturbance
is present in almost every other psychological disorder. Categories of affective disturbance:
Emotional reactivity problems
o Emotional intensity (over- / underreactions)
o Emotional duration (too short / long)
o Emotional frequency (too little / frequent)
o Emotion type (inappropriate)
Emotion regulation problems
o Awareness (Over or under)
o Goals (excessive dampening or searching for the peak)
o Strategies (Overuse or wrong implementation)
Typical approach over the last decades
Get patients with disorder A (defined by DSM) and healthy control group. Match groups carefully
on characteristics (age/ education level/ medication if possible). Compare them on affective
process X like amygdala response. Compare them on the process. Significance indicates a/no
substrate (foundering) for mental disorder.
When testing treatments, compare experimental treatment X v.s. control treatment Y.
significance indicates treatment efficacy.
But: Efficacy of psychological and pharmacological treatment for mental disorder is +/- 50%.
Possible reasons:
,The state of mental health science
Likely reasons for the lack of higher efficacy despite all the research:
1. Clinical heterogeneity
Psychiatric syndromes are hugely diverse: For depression, two patients could share only one
symptom e.g. 636.120 unique symptom profiles to match a diagnosis of PTSD !!!
2. Lack of mechanistic understanding
Lack of mechanistic specificity understanding precludes tailored treatment. Why are people
showing that disorder? With the flu we know what happens what is going wrong (mechanic)
but with depression we do not know.
Comorbidity and the need for a transdiagnostic perspective
There are often more diseases at once diagnosed (= comorbidity) Possible explanations:
Poor discriminant validity (DSM not specific enough)
One disorder may act as a risk factor for another
o Primary versus secondary disorder? (when young anxious can later on develop depression)
Common risk underlying of all these different disorders. Can emerge at different stages of the
disease:
o predisposing = the risk factors are there before the diagnostic threshold
o precipitating = specific event or trigger to the onset of the current problem
o perpetuating = maintain the problem once it has become established e.g. stress
The grouping of disorders by the DSM does not reflect a mechanistic
level
goals of DSM: develop a system to provide specific, reliable diagnosis based on clinical
experience.
Problem: this does not necessarily reflect the mechanism that we try to find with research
(mechanism = the way the problem developed, how is the problem triggerd?)
Scientific mechanistic research needs to focus on symptoms rather than syndromes (labels are
not specific enough, so start with the symptoms)
Result of the focus on the DSM
A gap between the goals of current clinical diagnosis and scientific studies
Research on one disorder is isolated from parallel research to other disorders
Diagnostic focus
The DSM has been the key driving force behind the current ‘disorder focus’
Advantages:
o Common language for communication between clinicians, scientists, etc.
Disadvantages
o A specific diagnosis can be at the cost of a complex clinical reality at the level of the patient
o Implicitly, the DSM treats each disorder as an independent, separated, entity
o Implicitly, it assumes that the disorders are abruptly distinct from ‘normal behavior’
o Arbitrary (random) cut-offs not so extremely evidence based as one would hope
Transdiagnostic focus
From diagnostic focus to a transdiagnostic focus
, focusing on processes that contribute to the aetiology (cause) and maintenance of symptoms
across diagnostic borders/disorders
functional approach
o Dissect the syndrome in component parts
o Focus on individual patient and central problematic behavior, specific tailored therapy
o focus on common processes of etiology or maintenance
Advantages of a transdiagnostic perspective
Could deal better with comorbidity
o On average, patients suffered from 2.1 disorders per person
o Point prevalence: 50% of patients with an anxiety disorder had at least one additional
anxiety disorder or depression
o Patients are rarely ‘pure’
o Overlap among patients within a diagnosis sometimes smaller than between
The heterogeneous disorders in the current diagnostic system are each made up of dysfunctional
versions of processes that vary along continua in the general population
o It’s more a continuum than heathy vs not view. Thinking of a scale.
o Compare the ‘abnormal’ versus ‘normal’ view of the DSM
o These dysfunctional processes are observed in a number of different disorders
Treatment development
o Greater transfer of theoretical and treatment advances across disorders
o Specify treatment components that are effective across disorders
Research Domain
Criteria (RDoC): a
different approach
RDoC: what is the
underlying mechanism
that causes the symptoms.
o Each symptom gets
independently
identify and traced
back to its neurobiological roots.
o Not looking into the labels but making categories based on data like genetic risk or brain
activity etc. then you can see what treatment works best.
Continuous approach
o describes behavior from normal to abnormal, instead of clincal diagnosis yes or no
RDoC works by looking at brain and behavior and then linking them to clinical symptoms. The
DSM and ICD works the other way around, first classifying clinical categories and then
determining what fits into those categories. RDoC includes a broader range of data such as
genetics, biology and physiology; the DSM and ICD only include symptom reports or
observations.
Criticism
o overly biology
, disadvantages and shortcoming of transdiagnostic perspective
divergent trajectories and multifiniality? See paper.
Literature week 1
Gross & Jazaieri (2014) – emotion, emotion regulation, and
psychopathology: an affective science perspective
Psychiatric disorders are not that specific with symptoms. Because of heterogeneity of emotion
related processes and the considerable divergence in the definitions of emotion and emotion
regulation. Also the heterogeneity within psychiatric disorders. Also the causal role of emotion and
emotion regulation difficulties is not clear. It is hard to precisely specify the emotion and emotion
regulation problems that characterize any given psychiatric disorder. But it is possible and vital to
clarify the links among emotion, emotion regulation and psychopathology.
Defining emotion and emotion regulation
Emotional reactivity = the changes in experiential, behavioral and physiological responses
because of the occurrence of emotions.
Modal model = perspective on how emotions arise and unfold.
Emotional-generative process = the situation that compels attention
evaluation of that situation multisystem response.
Emotion regulation occurs when one actives (implicit / explicit) a goal to influence the emotion –
generative process). It can take up many forms depending on the context:
intrinsic when regulating own emotions & extrinsic: someone else’s.
Three important common factors for adaptive regulation:
Awareness of emotions: that enhances the range of available strategies and the flexibility of
using them
Goals: increasing or decreasing the magnitude or intensity of emotion experience, expression or
physiology.
Strategies: executed to active the goals. Makes the means specific.
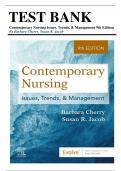
Five emotion-regulation processes
- Situation selection: influencing of you will
encounter a specific situation that is likely to
generate an emotion, desired or not
- Situation modification: alter external
features of the environment to influence
emotions
- Attentional deployment: (re)directing attention to alter emotional response
- Cognive change: to revise the meaning of the situation to influence one emotions
- Response modulation: efforts to made to influence one’s responses to the situation
Common to engage in behaviors that represent various combinations of different strategies rather
than a single isolated strategy in everyday life. Emotional-regulations can be adaptive or maladaptive
depending on individual emotion and context.
lecture notes
Week 1: Introduction lecture
Learning objectives
1. Summarize in what form affect and its regulation might be disrupted in psychopathological
processes
2. Reflect on the recent state of affairs and possible improvements in psychological clinical practice
by use of affective science.
3. Argue how transdiagnostic models can contribute to understanding origin and maintenance of
psychopathology, yet also come with potential challenges
Affective processes
Affect = involves an evaluation of a situation as salient (belangrijk) and thereby triggering an
evolutionary adaptive response. Consist of:
Subjective (negative or positive feeling) components
Behavioral (motor expression or inclination (neiging)) components
Physiological (brain/body) components
Affective science
= the scientific study of affective processes. Affected processes is an umbrella term.
- Event-focus = to what extent is the affective process coupled with an event.
- Embodiment = how strong is the physical component.
Affective disturbance
is present in almost every other psychological disorder. Categories of affective disturbance:
Emotional reactivity problems
o Emotional intensity (over- / underreactions)
o Emotional duration (too short / long)
o Emotional frequency (too little / frequent)
o Emotion type (inappropriate)
Emotion regulation problems
o Awareness (Over or under)
o Goals (excessive dampening or searching for the peak)
o Strategies (Overuse or wrong implementation)
Typical approach over the last decades
Get patients with disorder A (defined by DSM) and healthy control group. Match groups carefully
on characteristics (age/ education level/ medication if possible). Compare them on affective
process X like amygdala response. Compare them on the process. Significance indicates a/no
substrate (foundering) for mental disorder.
When testing treatments, compare experimental treatment X v.s. control treatment Y.
significance indicates treatment efficacy.
But: Efficacy of psychological and pharmacological treatment for mental disorder is +/- 50%.
Possible reasons:
,The state of mental health science
Likely reasons for the lack of higher efficacy despite all the research:
1. Clinical heterogeneity
Psychiatric syndromes are hugely diverse: For depression, two patients could share only one
symptom e.g. 636.120 unique symptom profiles to match a diagnosis of PTSD !!!
2. Lack of mechanistic understanding
Lack of mechanistic specificity understanding precludes tailored treatment. Why are people
showing that disorder? With the flu we know what happens what is going wrong (mechanic)
but with depression we do not know.
Comorbidity and the need for a transdiagnostic perspective
There are often more diseases at once diagnosed (= comorbidity) Possible explanations:
Poor discriminant validity (DSM not specific enough)
One disorder may act as a risk factor for another
o Primary versus secondary disorder? (when young anxious can later on develop depression)
Common risk underlying of all these different disorders. Can emerge at different stages of the
disease:
o predisposing = the risk factors are there before the diagnostic threshold
o precipitating = specific event or trigger to the onset of the current problem
o perpetuating = maintain the problem once it has become established e.g. stress
The grouping of disorders by the DSM does not reflect a mechanistic
level
goals of DSM: develop a system to provide specific, reliable diagnosis based on clinical
experience.
Problem: this does not necessarily reflect the mechanism that we try to find with research
(mechanism = the way the problem developed, how is the problem triggerd?)
Scientific mechanistic research needs to focus on symptoms rather than syndromes (labels are
not specific enough, so start with the symptoms)
Result of the focus on the DSM
A gap between the goals of current clinical diagnosis and scientific studies
Research on one disorder is isolated from parallel research to other disorders
Diagnostic focus
The DSM has been the key driving force behind the current ‘disorder focus’
Advantages:
o Common language for communication between clinicians, scientists, etc.
Disadvantages
o A specific diagnosis can be at the cost of a complex clinical reality at the level of the patient
o Implicitly, the DSM treats each disorder as an independent, separated, entity
o Implicitly, it assumes that the disorders are abruptly distinct from ‘normal behavior’
o Arbitrary (random) cut-offs not so extremely evidence based as one would hope
Transdiagnostic focus
From diagnostic focus to a transdiagnostic focus
, focusing on processes that contribute to the aetiology (cause) and maintenance of symptoms
across diagnostic borders/disorders
functional approach
o Dissect the syndrome in component parts
o Focus on individual patient and central problematic behavior, specific tailored therapy
o focus on common processes of etiology or maintenance
Advantages of a transdiagnostic perspective
Could deal better with comorbidity
o On average, patients suffered from 2.1 disorders per person
o Point prevalence: 50% of patients with an anxiety disorder had at least one additional
anxiety disorder or depression
o Patients are rarely ‘pure’
o Overlap among patients within a diagnosis sometimes smaller than between
The heterogeneous disorders in the current diagnostic system are each made up of dysfunctional
versions of processes that vary along continua in the general population
o It’s more a continuum than heathy vs not view. Thinking of a scale.
o Compare the ‘abnormal’ versus ‘normal’ view of the DSM
o These dysfunctional processes are observed in a number of different disorders
Treatment development
o Greater transfer of theoretical and treatment advances across disorders
o Specify treatment components that are effective across disorders
Research Domain
Criteria (RDoC): a
different approach
RDoC: what is the
underlying mechanism
that causes the symptoms.
o Each symptom gets
independently
identify and traced
back to its neurobiological roots.
o Not looking into the labels but making categories based on data like genetic risk or brain
activity etc. then you can see what treatment works best.
Continuous approach
o describes behavior from normal to abnormal, instead of clincal diagnosis yes or no
RDoC works by looking at brain and behavior and then linking them to clinical symptoms. The
DSM and ICD works the other way around, first classifying clinical categories and then
determining what fits into those categories. RDoC includes a broader range of data such as
genetics, biology and physiology; the DSM and ICD only include symptom reports or
observations.
Criticism
o overly biology
, disadvantages and shortcoming of transdiagnostic perspective
divergent trajectories and multifiniality? See paper.
Literature week 1
Gross & Jazaieri (2014) – emotion, emotion regulation, and
psychopathology: an affective science perspective
Psychiatric disorders are not that specific with symptoms. Because of heterogeneity of emotion
related processes and the considerable divergence in the definitions of emotion and emotion
regulation. Also the heterogeneity within psychiatric disorders. Also the causal role of emotion and
emotion regulation difficulties is not clear. It is hard to precisely specify the emotion and emotion
regulation problems that characterize any given psychiatric disorder. But it is possible and vital to
clarify the links among emotion, emotion regulation and psychopathology.
Defining emotion and emotion regulation
Emotional reactivity = the changes in experiential, behavioral and physiological responses
because of the occurrence of emotions.
Modal model = perspective on how emotions arise and unfold.
Emotional-generative process = the situation that compels attention
evaluation of that situation multisystem response.
Emotion regulation occurs when one actives (implicit / explicit) a goal to influence the emotion –
generative process). It can take up many forms depending on the context:
intrinsic when regulating own emotions & extrinsic: someone else’s.
Three important common factors for adaptive regulation:
Awareness of emotions: that enhances the range of available strategies and the flexibility of
using them
Goals: increasing or decreasing the magnitude or intensity of emotion experience, expression or
physiology.
Strategies: executed to active the goals. Makes the means specific.
Five emotion-regulation processes
- Situation selection: influencing of you will
encounter a specific situation that is likely to
generate an emotion, desired or not
- Situation modification: alter external
features of the environment to influence
emotions
- Attentional deployment: (re)directing attention to alter emotional response
- Cognive change: to revise the meaning of the situation to influence one emotions
- Response modulation: efforts to made to influence one’s responses to the situation
Common to engage in behaviors that represent various combinations of different strategies rather
than a single isolated strategy in everyday life. Emotional-regulations can be adaptive or maladaptive
depending on individual emotion and context.