NUR 505 Advanced Health Assessment
Module 3 Vital Signs, Pain, and Mental Status Study Guide
Chapter 6 Vital Signs and Pain
1. Define the following terms:
• Blood Pressure:
o The arterial blood pressure is the force of blood against the wall of an artery
as the ventricles of the heart contract and relax.
o Systolic BP is the force exerted when the ventricles contract, is largely the
result of cardiac output, blood volume, and compliance of the arteries.
o Diastolic pressure is the force exerted by peripheral vascular resistance when
the heart is in the filling or relaxed state. Blood pressure is highest during
systole and falls to the lowest point during diastole.
o The pulse pressure is the difference between the systolic and diastolic
pressures.
▪ Healthy: < 120/80
▪ Elevated/ Pre-hypertensive: SBP 120-129 & DBP < 80
▪ Hypertension stage 1: SBP 103-139 or DBP 80-89
▪ Hypertension stage 2: SBP >140 or DBP > 90
• Nonverbal Pain Indicators:
• Facial Expressions:
o Grimacing or wincing.
o Furrowed brows or a tense facial expression.
o Clenched teeth or a tightened jaw.
o Frequent blinking or rapid eye movements.
• Body Language:
o Restlessness or constant shifting in bed or chair.
o Guarding or protecting a specific body part.
o Fidgeting or pacing.
o Changes in posture, such as leaning forward or hunching over.
• Vocalizations:
o Moaning or groaning.
o Crying or whimpering.
o Sighing heavily or making distressed sounds.
• Changes in Breathing:
o Rapid or shallow breathing.
o Holding one's breath during movement or when touched.
, o Labored breathing.
• Agitation and Irritability:
o Increased agitation or irritability, especially in someone who is usually calm.
o Aggressive behavior or resistance to care.
• Changes in Vital Signs:
o Increased heart rate (tachycardia).
o Increased blood pressure.
o Increased respiratory rate (tachypnea).
• Altered Sleep Patterns:
o Difficulty falling asleep or staying asleep.
o Frequent awakening during the night.
• Changes in Eating Habits:
o Reduced appetite or refusal to eat.
o Changes in swallowing patterns or difficulty swallowing.
• Skin Changes:
o Pallor (paleness) or flushing (redness) of the skin.
o Sweating or clammy skin.
o Increased muscle tension or rigidity.
• Gait and Mobility Changes:
o Slow or hesitant movements.
o Changes in walking pattern, such as limping or shuffling.
• Eyes and Gaze:
o Avoiding eye contact.
o A fixed or distant stare.
• Changes in Social Behavior:
o Withdrawal from social interactions.
o Loss of interest in usual activities.
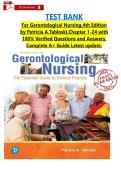
▪ Healthcare providers may use pain assessment tools specifically
designed for individuals who have difficulty expressing pain verbally,
such as the Wong-Baker FACES Pain Rating Scale or the Non-
Communicating Children's Pain Checklist (NCCPC). These tools can
help quantify pain severity and guide appropriate interventions.
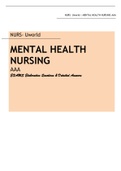
, ***Nonverbal children can use the FLACC Behavioral Pain Assessment Scale***
FLACC is an acronym for the five assessment categories: face, legs, activity, cry, and
consolability. This scale is used most commonly to assess acute pain associated with surgery in
children between 2 months and 7 years of age.
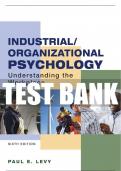
• Korotkoff sounds- low-pitched sound produced by the turbulence of blood flow in
the artery *Best heard with the bell of a stethoscope*
o Two consecutive beats indicate the systolic pressure reading, and the
beginning of Korotkoff sounds, phase 1.
o Sometimes the Korotkoff sounds will be heard, then disappear, and then
reappear 10 to 15 mm Hg below the systolic pressure reading (Korotkoff
sounds, phase 2).
o The period of silence is the auscultatory gap.
o Be aware of the possibility of this gap to avoid underestimation of the
systolic pressure or overestimation of the diastolic pressure.
o The auscultatory gap widens with systolic hypertension in older persons due
to the loss of arterial pliability. It also widens with a drop in diastolic pressure
when chronic severe aortic regurgitation is present.
o The auscultatory gap narrows in the case of pulsus paradoxus due to cardiac
tamponade or other constrictive cardiac events.
o Note the point at which the initial crisp sounds (Korotkoff sounds, phase 3)
become muffled (Korotkoff sounds, phase 4). The muffled sound is the first
diastolic sound, and it is the closest approximation of direct diastolic arterial
pressure. It signals the disappearance of the Korotkoff sounds.
Module 3 Vital Signs, Pain, and Mental Status Study Guide
Chapter 6 Vital Signs and Pain
1. Define the following terms:
• Blood Pressure:
o The arterial blood pressure is the force of blood against the wall of an artery
as the ventricles of the heart contract and relax.
o Systolic BP is the force exerted when the ventricles contract, is largely the
result of cardiac output, blood volume, and compliance of the arteries.
o Diastolic pressure is the force exerted by peripheral vascular resistance when
the heart is in the filling or relaxed state. Blood pressure is highest during
systole and falls to the lowest point during diastole.
o The pulse pressure is the difference between the systolic and diastolic
pressures.
▪ Healthy: < 120/80
▪ Elevated/ Pre-hypertensive: SBP 120-129 & DBP < 80
▪ Hypertension stage 1: SBP 103-139 or DBP 80-89
▪ Hypertension stage 2: SBP >140 or DBP > 90
• Nonverbal Pain Indicators:
• Facial Expressions:
o Grimacing or wincing.
o Furrowed brows or a tense facial expression.
o Clenched teeth or a tightened jaw.
o Frequent blinking or rapid eye movements.
• Body Language:
o Restlessness or constant shifting in bed or chair.
o Guarding or protecting a specific body part.
o Fidgeting or pacing.
o Changes in posture, such as leaning forward or hunching over.
• Vocalizations:
o Moaning or groaning.
o Crying or whimpering.
o Sighing heavily or making distressed sounds.
• Changes in Breathing:
o Rapid or shallow breathing.
o Holding one's breath during movement or when touched.
, o Labored breathing.
• Agitation and Irritability:
o Increased agitation or irritability, especially in someone who is usually calm.
o Aggressive behavior or resistance to care.
• Changes in Vital Signs:
o Increased heart rate (tachycardia).
o Increased blood pressure.
o Increased respiratory rate (tachypnea).
• Altered Sleep Patterns:
o Difficulty falling asleep or staying asleep.
o Frequent awakening during the night.
• Changes in Eating Habits:
o Reduced appetite or refusal to eat.
o Changes in swallowing patterns or difficulty swallowing.
• Skin Changes:
o Pallor (paleness) or flushing (redness) of the skin.
o Sweating or clammy skin.
o Increased muscle tension or rigidity.
• Gait and Mobility Changes:
o Slow or hesitant movements.
o Changes in walking pattern, such as limping or shuffling.
• Eyes and Gaze:
o Avoiding eye contact.
o A fixed or distant stare.
• Changes in Social Behavior:
o Withdrawal from social interactions.
o Loss of interest in usual activities.
▪ Healthcare providers may use pain assessment tools specifically
designed for individuals who have difficulty expressing pain verbally,
such as the Wong-Baker FACES Pain Rating Scale or the Non-
Communicating Children's Pain Checklist (NCCPC). These tools can
help quantify pain severity and guide appropriate interventions.
, ***Nonverbal children can use the FLACC Behavioral Pain Assessment Scale***
FLACC is an acronym for the five assessment categories: face, legs, activity, cry, and
consolability. This scale is used most commonly to assess acute pain associated with surgery in
children between 2 months and 7 years of age.
• Korotkoff sounds- low-pitched sound produced by the turbulence of blood flow in
the artery *Best heard with the bell of a stethoscope*
o Two consecutive beats indicate the systolic pressure reading, and the
beginning of Korotkoff sounds, phase 1.
o Sometimes the Korotkoff sounds will be heard, then disappear, and then
reappear 10 to 15 mm Hg below the systolic pressure reading (Korotkoff
sounds, phase 2).
o The period of silence is the auscultatory gap.
o Be aware of the possibility of this gap to avoid underestimation of the
systolic pressure or overestimation of the diastolic pressure.
o The auscultatory gap widens with systolic hypertension in older persons due
to the loss of arterial pliability. It also widens with a drop in diastolic pressure
when chronic severe aortic regurgitation is present.
o The auscultatory gap narrows in the case of pulsus paradoxus due to cardiac
tamponade or other constrictive cardiac events.
o Note the point at which the initial crisp sounds (Korotkoff sounds, phase 3)
become muffled (Korotkoff sounds, phase 4). The muffled sound is the first
diastolic sound, and it is the closest approximation of direct diastolic arterial
pressure. It signals the disappearance of the Korotkoff sounds.