Cardiovascular Dysrhythmia Concepts
Care of Patients with Dysrhythmias
Key Learning Objectives
Safe and Effective Care Environment.
1. Collaborate with the interprofessional team to coordinate high-quality care to promote PERFUSION in patients with dysrhythmias.
2. Provide a safe environment for patients and staff when using a cardiac defibrillator.
Health Promotion and Maintenance.
1. Teach the patient and caregiver(s) about drug therapy used for common dysrhythmias.
2. Teach the patient with a pacemaker or implantable cardioverter/defibrillator about self-management when in the community.
Psychosocial Integrity.
1. Implement patient and family-centered nursing interventions to decrease the psychosocial impact caused by life-threatening dysrhythmias and emergency care
procedures.
Physiological Integrity.
1. Apply knowledge of pathophysiology to assess patients with common dysrhythmias.
2. Analyze an ECG rhythm strip to identify normal sinus rhythm and common or life-threatening dysrhythmias.
3. Use clinical judgment to plan care coordination and transition management for patients experiencing common dysrhythmias.
4. Plan evidence-based nursing care to promote PERFUSION to prevent complications in patients experiencing dysrhythmias.
5. Explain the need to perform evidence-based emergency care procedures, such as cardiopulmonary resuscitation (CPR) and automated external defibrillation.
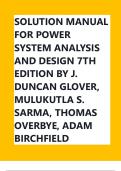
Rhythm Waveform Analysis
Rate Analysis Notes: Each segment between the dark lines (above the monitor strip) represents 3 seconds when the monitor is set at a speed of 25 mm per second. To estimate
the ventricular rate, count the QRS complexes in a 6-second strip and multiply that number by 10 to estimate the rate for 1 minute. In this example, there are 9 QRS complexes
in 6 seconds. Therefore the heart rate can be estimated to be 90 beats/min.
Page 1 of 17
Ignatavicius, et al, Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 9 th Edition, ELSEVIER, 2018
,Cardiovascular Dysrhythmia Concepts
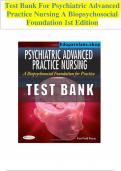
Electrocardiographic Complexes, Segments, and Intervals Notes: Complexes that make up a normal ECG consist of a P wave, a QRS complex, a T wave, and
possibly a U wave. Segments include the PR segment, the ST segment, and the TP segment. Intervals include the PR interval, the QRS duration, and the QT
interval (see below)
Page 2 of 17
Ignatavicius, et al, Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 9 th Edition, ELSEVIER, 2018
, Cardiovascular Dysrhythmia Concepts
Wave Components
The P wave is a deflection representing atrial depolarization. The shape of the P wave may be a positive, negative, or biphasic (both positive and
negative) deflection, depending on the lead selected. When the electrical impulse is consistently generated from the sinoatrial (SA) node, the P
waves have a consistent shape in a given lead. If an impulse is then generated from a different (ectopic) focus, such as atrial tissue, the shape of
the P wave changes in that lead, indicating that an ectopic focus has fired.
The PR segment is the isoelectric line from the end of the P wave to the beginning of the QRS complex, when the electrical impulse is traveling
through the atrioventricular (AV) node, where it is delayed. It then travels through the ventricular conduction system to the Purkinje fibers.
The PR interval is measured from the beginning of the P wave to the end of the PR segment. It represents the time required for atrial depolarization,
the impulse delay in the AV node, and the travel time to the Purkinje fibers. It normally measures from 0.12 to 0.20 second (five small blocks).
The QRS complex represents ventricular depolarization. The shape of the QRS complex depends on the lead selected. The Q wave is the first
negative deflection and is not present in all leads. When present, it is small and represents initial ventricular septal depolarization. When the Q wave
is abnormally present in a lead, it represents myocardial necrosis (cell death).
The R wave is the first positive deflection. It may be small, large, or absent, depending on the lead.
The S wave is a negative deflection following the R wave and is not present in all leads.
The QRS duration represents the time required for depolarization of both ventricles. It is measured from the beginning of the QRS complex to the J
point (the junction where the QRS complex ends and the ST segment begins). It normally measures from 0.04 to 0.12 second (up to three small
blocks).
The ST segment is normally an isoelectric line and represents early ventricular repolarization. It occurs from the J point to the beginning of the T
wave. Its length varies with changes in the heart rate, the administration of medications, and electrolyte disturbances.
The T wave follows the ST segment and represents ventricular repolarization. It is usually positive, rounded, and slightly asymmetric. T waves may
become tall and peaked; inverted (negative); or flat as a result of myocardial ischemia, potassium or calcium imbalances, medications, or
autonomic nervous system effects.
The U wave, when present, follows the T wave and may result from slow repolarization of ventricular Purkinje fibers. It is of the same polarity as the
T wave, although generally it is smaller. It is not normally seen in all leads and is more common in lead V3. An abnormal U wave may suggest an
Page 3 of 17
Ignatavicius, et al, Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 9 th Edition, ELSEVIER, 2018
Care of Patients with Dysrhythmias
Key Learning Objectives
Safe and Effective Care Environment.
1. Collaborate with the interprofessional team to coordinate high-quality care to promote PERFUSION in patients with dysrhythmias.
2. Provide a safe environment for patients and staff when using a cardiac defibrillator.
Health Promotion and Maintenance.
1. Teach the patient and caregiver(s) about drug therapy used for common dysrhythmias.
2. Teach the patient with a pacemaker or implantable cardioverter/defibrillator about self-management when in the community.
Psychosocial Integrity.
1. Implement patient and family-centered nursing interventions to decrease the psychosocial impact caused by life-threatening dysrhythmias and emergency care
procedures.
Physiological Integrity.
1. Apply knowledge of pathophysiology to assess patients with common dysrhythmias.
2. Analyze an ECG rhythm strip to identify normal sinus rhythm and common or life-threatening dysrhythmias.
3. Use clinical judgment to plan care coordination and transition management for patients experiencing common dysrhythmias.
4. Plan evidence-based nursing care to promote PERFUSION to prevent complications in patients experiencing dysrhythmias.
5. Explain the need to perform evidence-based emergency care procedures, such as cardiopulmonary resuscitation (CPR) and automated external defibrillation.
Rhythm Waveform Analysis
Rate Analysis Notes: Each segment between the dark lines (above the monitor strip) represents 3 seconds when the monitor is set at a speed of 25 mm per second. To estimate
the ventricular rate, count the QRS complexes in a 6-second strip and multiply that number by 10 to estimate the rate for 1 minute. In this example, there are 9 QRS complexes
in 6 seconds. Therefore the heart rate can be estimated to be 90 beats/min.
Page 1 of 17
Ignatavicius, et al, Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 9 th Edition, ELSEVIER, 2018
,Cardiovascular Dysrhythmia Concepts
Electrocardiographic Complexes, Segments, and Intervals Notes: Complexes that make up a normal ECG consist of a P wave, a QRS complex, a T wave, and
possibly a U wave. Segments include the PR segment, the ST segment, and the TP segment. Intervals include the PR interval, the QRS duration, and the QT
interval (see below)
Page 2 of 17
Ignatavicius, et al, Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 9 th Edition, ELSEVIER, 2018
, Cardiovascular Dysrhythmia Concepts
Wave Components
The P wave is a deflection representing atrial depolarization. The shape of the P wave may be a positive, negative, or biphasic (both positive and
negative) deflection, depending on the lead selected. When the electrical impulse is consistently generated from the sinoatrial (SA) node, the P
waves have a consistent shape in a given lead. If an impulse is then generated from a different (ectopic) focus, such as atrial tissue, the shape of
the P wave changes in that lead, indicating that an ectopic focus has fired.
The PR segment is the isoelectric line from the end of the P wave to the beginning of the QRS complex, when the electrical impulse is traveling
through the atrioventricular (AV) node, where it is delayed. It then travels through the ventricular conduction system to the Purkinje fibers.
The PR interval is measured from the beginning of the P wave to the end of the PR segment. It represents the time required for atrial depolarization,
the impulse delay in the AV node, and the travel time to the Purkinje fibers. It normally measures from 0.12 to 0.20 second (five small blocks).
The QRS complex represents ventricular depolarization. The shape of the QRS complex depends on the lead selected. The Q wave is the first
negative deflection and is not present in all leads. When present, it is small and represents initial ventricular septal depolarization. When the Q wave
is abnormally present in a lead, it represents myocardial necrosis (cell death).
The R wave is the first positive deflection. It may be small, large, or absent, depending on the lead.
The S wave is a negative deflection following the R wave and is not present in all leads.
The QRS duration represents the time required for depolarization of both ventricles. It is measured from the beginning of the QRS complex to the J
point (the junction where the QRS complex ends and the ST segment begins). It normally measures from 0.04 to 0.12 second (up to three small
blocks).
The ST segment is normally an isoelectric line and represents early ventricular repolarization. It occurs from the J point to the beginning of the T
wave. Its length varies with changes in the heart rate, the administration of medications, and electrolyte disturbances.
The T wave follows the ST segment and represents ventricular repolarization. It is usually positive, rounded, and slightly asymmetric. T waves may
become tall and peaked; inverted (negative); or flat as a result of myocardial ischemia, potassium or calcium imbalances, medications, or
autonomic nervous system effects.
The U wave, when present, follows the T wave and may result from slow repolarization of ventricular Purkinje fibers. It is of the same polarity as the
T wave, although generally it is smaller. It is not normally seen in all leads and is more common in lead V3. An abnormal U wave may suggest an
Page 3 of 17
Ignatavicius, et al, Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 9 th Edition, ELSEVIER, 2018