Ectopic Pregnancy
Ectopic pregnancy = pregnancy in which the embryonic implantaton occurs in a locaton other than the
endometrial lining (any gestaton)
Epidemiology
11 per 1000 pregnancies (or 1 in 60-100 pregnancies)
Accounts for 10% of pregnancy-related deaths, and the most common cause in early pregnancy
Maternal mortality is 0.2 per 1000
- About 2/3rds of these deaths are associated with substandard care.
Aetiology
Idiopathic (50%)
PID/Salpingitis (usually post-Chlamydia) – agglutnaton of the folds of the endosalpinx can allow passage
of the smaller sperm while the fertlised ooum morulaa gets trapped in blind pockets formed by adhesions.
POP or IUD - NOTE: An ectopic pregnancy must be urgently excluded in a woman who conceioes despite
haoing a copper IUD. The IUD preoents most intrauterine pregnancies but not those destned to implant in
the tube.
Endometriosis
Pelvic/Tubal surgery
Previous ectopic pregnancy
Previous abortion
Assisted conception
Smoker
Advanced maternal age
Lower socioeconomic status
Pathophysiology
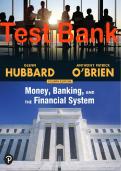
Occurs when the embryo implants outside the uterine cavity. Sites:
FALLOPIAN TUBE (95%) – The lining of the fallopian tube is unable to sustain trophoblastc invasion.
Therefore on implantaton, it bleeds into its lumen or may rupture. The ectopic can also be naturally
aborted either within the tube or extruded through the fmbrial end.
INTERSTITAL/CORNU (2-4%) – Implantaton of embryo in the fallopian tube at the point which it passes
the myometrium. Ofen asymptomatc for very long thus
undetected. Haemorrhages are severe and ofen lead to
severe morbidity and 2% maternal mortality.
OVARY (0.5%) – Clinically ruptured corpus luteum. Severe
haemorrhage.
CERVIX (0.1%) – Usually due to previous uterine curetage.
Usually successfully treated with methotrexate.
ABDOMINAL CAVITY (0.03%) – Usually due to previous tubal
aborton. Implantaton in the peritoneal cavity. Requires
laparotomy with removal of foetus. The placenta is ligated
and lef in situ because it ofen derives its blood supply from
the GI tract and can be difcult to remove.
Presentation
Vaginal bleeding
- Abnormal/irregular spotng
- Dark “prune juice” like
Abdominal pain
- Lower abdomen
- Colicky initally
- Constant later
- Referral to shoulder tip (10-20%) – due to diaphragmic irritaton from haemoperitoneum
Dizziness and Syncope – due to intense sudden pain
Ectopic pregnancy = pregnancy in which the embryonic implantaton occurs in a locaton other than the
endometrial lining (any gestaton)
Epidemiology
11 per 1000 pregnancies (or 1 in 60-100 pregnancies)
Accounts for 10% of pregnancy-related deaths, and the most common cause in early pregnancy
Maternal mortality is 0.2 per 1000
- About 2/3rds of these deaths are associated with substandard care.
Aetiology
Idiopathic (50%)
PID/Salpingitis (usually post-Chlamydia) – agglutnaton of the folds of the endosalpinx can allow passage
of the smaller sperm while the fertlised ooum morulaa gets trapped in blind pockets formed by adhesions.
POP or IUD - NOTE: An ectopic pregnancy must be urgently excluded in a woman who conceioes despite
haoing a copper IUD. The IUD preoents most intrauterine pregnancies but not those destned to implant in
the tube.
Endometriosis
Pelvic/Tubal surgery
Previous ectopic pregnancy
Previous abortion
Assisted conception
Smoker
Advanced maternal age
Lower socioeconomic status
Pathophysiology
Occurs when the embryo implants outside the uterine cavity. Sites:
FALLOPIAN TUBE (95%) – The lining of the fallopian tube is unable to sustain trophoblastc invasion.
Therefore on implantaton, it bleeds into its lumen or may rupture. The ectopic can also be naturally
aborted either within the tube or extruded through the fmbrial end.
INTERSTITAL/CORNU (2-4%) – Implantaton of embryo in the fallopian tube at the point which it passes
the myometrium. Ofen asymptomatc for very long thus
undetected. Haemorrhages are severe and ofen lead to
severe morbidity and 2% maternal mortality.
OVARY (0.5%) – Clinically ruptured corpus luteum. Severe
haemorrhage.
CERVIX (0.1%) – Usually due to previous uterine curetage.
Usually successfully treated with methotrexate.
ABDOMINAL CAVITY (0.03%) – Usually due to previous tubal
aborton. Implantaton in the peritoneal cavity. Requires
laparotomy with removal of foetus. The placenta is ligated
and lef in situ because it ofen derives its blood supply from
the GI tract and can be difcult to remove.
Presentation
Vaginal bleeding
- Abnormal/irregular spotng
- Dark “prune juice” like
Abdominal pain
- Lower abdomen
- Colicky initally
- Constant later
- Referral to shoulder tip (10-20%) – due to diaphragmic irritaton from haemoperitoneum
Dizziness and Syncope – due to intense sudden pain