Gut-brain axis in Parkinson’s disease (Prof.
De Schepper)
1. Parkinson’s disease
1.1. PD causes major disability related to motor and non-
motor symptoms
Motor symptoms: patients that suffer from severe symptoms making it
difficult to move
o Bradykinesia
o Tremors
o Rigidity
Symptoms that are not related to your movement = non-motor
symptoms
o Depression
o Sense of smell
o Joint pain
1.2. PD is caused by the selective loss of dopaminergic cells in
the Substantia Nigra Pars Compacta (SNpc)
The pars compacta region of the SNpc modulates the activity of the
striatum, via the neurotransmitter, dopamine - this modulation is critical
in the control of body movement
At the microscopic level, there is marked and selective degeneration of
dopaminergic neurons in the substantia nigra in PD
In a PD patient the dopamine neurons are gone this causes the typical
symptoms of PD
Neuronal cell death within the substantia nigra is reflected by the loss of
neuromelanin pigmentation
1.3. α -synuclein is the pathological hallmark of PD
Normally existing in a soluble, unfolded form, in PD α -synuclein aggregates
into fibrils to form Lewy bodies
α -synuclein aggregation is thought to be driven by many genetic variations
associated with PD
1
, α -synuclein seems to be key to the disease process in most if not all cases of
idiopathic PD; however, some monogenic forms of PD appear to lack
synucleinopathy (e.g. a proportion of cases related to PRKN or LRRK2)
α -synuclein is a target for developing treatments for PD
o Many of the disease-modifying treatments for PD under investigation
target α -synuclein aggregation
1.3.1. α -synuclein pathology progresses according to the Braak staging
PD is hypothesized to progress in six neuropathological stages: Braak
Stages
o Braak stage 1-2: autonomic and olfactory disturbances
o Braak stages 3-4: sleep and motor disturbances
o Braak stages 5-6: emotional and cognitive disturbances
All of the affected neurons eventually develop Lewy pathology, but, despite
the presence of inclusion bodies, some neurons survive for a long period of
time
PD is a progressive disorder
Pathology might start somewhere and overtime it will spread/transmit from
one brain region to another
α -synuclein follows a certain pattern over the years
At very early stage it appears in the brain stem
Not all neurons will degenerate in this region some neurons are
protected
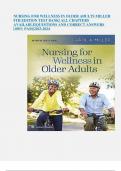
1.3.2. α -synuclein pathology spreads from cell to cell
Potential mechanisms for the spreading of α-synuclein. Pathological
proteins, or ‘seeds’, are released from donor cells and might be taken up
by recipient neurons
(a) Receptor-mediated endocytosis
(b) direct penetration of the plasma membrane
(c) or fluid-phase endocytosis
(d) fusion of vesicles with the plasma membrane
2
, (e) tunnelling nanotubes that directly
connect the two cells
The transmission process can be
modulated by multiple factors, including
the clearance of α-synuclein by immune
cells.
Aggregation of α-synuclein is thought to
result from failure of its clearance
1.3.3. α -synuclein causes toxicity to the
endolysosomal and mitochondrial components of the cell
Genes associated with PD development point to the importance of
mitochondrial dysfunction, oxidative stress, lipid metabolism and
lysosomal dysfunction in the pathogenesis of PD.
Many of the genes are in fact expressed in immune cells, in particular:
Myeloid cells (monocytes, macrophages, microglia)
1.4. New strategies are needed to slow down disease
progression in the prodromal phase
Prodromal phase = no motor symptoms yet but disease started showing
symptoms in other parts
At the time of diagnosis (year 0), already 60-70% of the dopaminergic
neurons in the SNpc have been degenerated.
o The disease is irreversible therapy is too late so try to tackle
the disease from
an earlier
timepoint
It is critically important
to develop therapeutic
strategies to prevent
further neuron loss and
to prevent the formation
of Lewy pathology in
other brain areas.
Possible strategies:
o Prevent initial
aggregation of α-
synuclein
o Improve clearance
of α-synuclein
o Prevent spreading
of α-synuclein
1.5. Conclusions
PD is a neurodegenerative disorder associated with the deposition of
aggregated α-synuclein
3
, Abnormal aggregation and cell-cell spreading of α-synuclein between the
gut, brainstem, and higher brain regions underlie the development and
progression of pathology
Dysfunctional mitochondrial, lysosomal, and endosomal pathways are
involved in its pathogenesis, leading to a complex cascade of
neuroinflammation, synaptic dysfunction and neurodegeneration
The disease is characterized by a prodromal phase, where
neurodegeneration might still be reversible
The important challenge is to better characterize the prodromal
phase The failure of trials of disease-modifying interventions in PD to date
may in part be due to the fact that pathology in established PD is too
advanced for the treatments to be effective..
2. Potential gut origins of disease
2.1. The distribution of α -synuclein pathology is not restricted
to the brain
α-synuclein deposition has been detected in biopsies from the oesophagus,
stomach, small intestine and colon up to 20 years before PD diagnosis
It is suggested that PD may originate in the enteric nervous system (ENS) –
the so-called ‘little brain of the gut’, and its pathological progression in the
brain may be mediated by the prion-like properties of α-synuclein
Many patients suffer from constipation and other gut dysfunctions,
potentially linked to α-synuclein-associated ENS dysfunctions
Inflammatory bowel disease (20-90% increased risk for developing PD)
2.2. The ENS has multiple roles that are crucial for gut
function
Intricate networks of un-myelinated nerve fibers intermingled with clusters
of neuronal cell bodies (=ganglia), glia and immune cells
2 major structures: Myenteric plexus and Submucosal plexus (SMP)
Its key functions: muscle activity, secretion, absorption, regulating blood
flow, interacting with the immune system of the gut
The ENS does not need input from the CNS for its functioning
The myenteric plexus projects to the dorsal motor nucleus of the vagus
(DMV) in the brainstem via the vagus nerve
4
,2.3. The gut-brain neural connection
5
, 2.4. PD and α -synuclein pathology in the ENS
Mounting evidence suggests that diseases affecting the CNS could have a
similar pathogenesis in the ENS – one theory holds that insults to the GI
tract may result in α-synuclein pathology in the ENS, which then ascends
along the gut-brain axis to the brain
It is unclear whether α-synuclein pathology begins ‘brain-first’ or ‘gut-first’,
or whether both processes exist within the PD population
The detection of ENS pathology may therefore be potentially useful for the
diagnosis or monitoring of PD, and add to the exciting prospect of
preventing or delaying the onset of PD
2.4.1. PD and α -synuclein pathology in the ENS: evidence from genetic
studies
Genetic risk for PD maps mainly to enteric neurons.
Among all nervous-system cell types analyzed, enteric neurons show
significant enrichment of PD-associated genes.
This suggests that the ENS is a genetically relevant site for PD
pathogenesis, consistent with gut-first models.
Even after adjusting for other neuronal populations, enteric neurons retain
an independent PD genetic signal, indicating a true contribution rather
than spill-over from CNS neurons.
2.5. PD and the gut-brain (or brain-gut) axis
Brain-first = the α-synuclein pathology of PD could begin in the brain and
then spread to the brainstem and the rest of the body
Body-first = the α-synuclein pathology could first arise somewhere in the
body, such as the gut, and then spreads upwards to the brain
6
De Schepper)
1. Parkinson’s disease
1.1. PD causes major disability related to motor and non-
motor symptoms
Motor symptoms: patients that suffer from severe symptoms making it
difficult to move
o Bradykinesia
o Tremors
o Rigidity
Symptoms that are not related to your movement = non-motor
symptoms
o Depression
o Sense of smell
o Joint pain
1.2. PD is caused by the selective loss of dopaminergic cells in
the Substantia Nigra Pars Compacta (SNpc)
The pars compacta region of the SNpc modulates the activity of the
striatum, via the neurotransmitter, dopamine - this modulation is critical
in the control of body movement
At the microscopic level, there is marked and selective degeneration of
dopaminergic neurons in the substantia nigra in PD
In a PD patient the dopamine neurons are gone this causes the typical
symptoms of PD
Neuronal cell death within the substantia nigra is reflected by the loss of
neuromelanin pigmentation
1.3. α -synuclein is the pathological hallmark of PD
Normally existing in a soluble, unfolded form, in PD α -synuclein aggregates
into fibrils to form Lewy bodies
α -synuclein aggregation is thought to be driven by many genetic variations
associated with PD
1
, α -synuclein seems to be key to the disease process in most if not all cases of
idiopathic PD; however, some monogenic forms of PD appear to lack
synucleinopathy (e.g. a proportion of cases related to PRKN or LRRK2)
α -synuclein is a target for developing treatments for PD
o Many of the disease-modifying treatments for PD under investigation
target α -synuclein aggregation
1.3.1. α -synuclein pathology progresses according to the Braak staging
PD is hypothesized to progress in six neuropathological stages: Braak
Stages
o Braak stage 1-2: autonomic and olfactory disturbances
o Braak stages 3-4: sleep and motor disturbances
o Braak stages 5-6: emotional and cognitive disturbances
All of the affected neurons eventually develop Lewy pathology, but, despite
the presence of inclusion bodies, some neurons survive for a long period of
time
PD is a progressive disorder
Pathology might start somewhere and overtime it will spread/transmit from
one brain region to another
α -synuclein follows a certain pattern over the years
At very early stage it appears in the brain stem
Not all neurons will degenerate in this region some neurons are
protected
1.3.2. α -synuclein pathology spreads from cell to cell
Potential mechanisms for the spreading of α-synuclein. Pathological
proteins, or ‘seeds’, are released from donor cells and might be taken up
by recipient neurons
(a) Receptor-mediated endocytosis
(b) direct penetration of the plasma membrane
(c) or fluid-phase endocytosis
(d) fusion of vesicles with the plasma membrane
2
, (e) tunnelling nanotubes that directly
connect the two cells
The transmission process can be
modulated by multiple factors, including
the clearance of α-synuclein by immune
cells.
Aggregation of α-synuclein is thought to
result from failure of its clearance
1.3.3. α -synuclein causes toxicity to the
endolysosomal and mitochondrial components of the cell
Genes associated with PD development point to the importance of
mitochondrial dysfunction, oxidative stress, lipid metabolism and
lysosomal dysfunction in the pathogenesis of PD.
Many of the genes are in fact expressed in immune cells, in particular:
Myeloid cells (monocytes, macrophages, microglia)
1.4. New strategies are needed to slow down disease
progression in the prodromal phase
Prodromal phase = no motor symptoms yet but disease started showing
symptoms in other parts
At the time of diagnosis (year 0), already 60-70% of the dopaminergic
neurons in the SNpc have been degenerated.
o The disease is irreversible therapy is too late so try to tackle
the disease from
an earlier
timepoint
It is critically important
to develop therapeutic
strategies to prevent
further neuron loss and
to prevent the formation
of Lewy pathology in
other brain areas.
Possible strategies:
o Prevent initial
aggregation of α-
synuclein
o Improve clearance
of α-synuclein
o Prevent spreading
of α-synuclein
1.5. Conclusions
PD is a neurodegenerative disorder associated with the deposition of
aggregated α-synuclein
3
, Abnormal aggregation and cell-cell spreading of α-synuclein between the
gut, brainstem, and higher brain regions underlie the development and
progression of pathology
Dysfunctional mitochondrial, lysosomal, and endosomal pathways are
involved in its pathogenesis, leading to a complex cascade of
neuroinflammation, synaptic dysfunction and neurodegeneration
The disease is characterized by a prodromal phase, where
neurodegeneration might still be reversible
The important challenge is to better characterize the prodromal
phase The failure of trials of disease-modifying interventions in PD to date
may in part be due to the fact that pathology in established PD is too
advanced for the treatments to be effective..
2. Potential gut origins of disease
2.1. The distribution of α -synuclein pathology is not restricted
to the brain
α-synuclein deposition has been detected in biopsies from the oesophagus,
stomach, small intestine and colon up to 20 years before PD diagnosis
It is suggested that PD may originate in the enteric nervous system (ENS) –
the so-called ‘little brain of the gut’, and its pathological progression in the
brain may be mediated by the prion-like properties of α-synuclein
Many patients suffer from constipation and other gut dysfunctions,
potentially linked to α-synuclein-associated ENS dysfunctions
Inflammatory bowel disease (20-90% increased risk for developing PD)
2.2. The ENS has multiple roles that are crucial for gut
function
Intricate networks of un-myelinated nerve fibers intermingled with clusters
of neuronal cell bodies (=ganglia), glia and immune cells
2 major structures: Myenteric plexus and Submucosal plexus (SMP)
Its key functions: muscle activity, secretion, absorption, regulating blood
flow, interacting with the immune system of the gut
The ENS does not need input from the CNS for its functioning
The myenteric plexus projects to the dorsal motor nucleus of the vagus
(DMV) in the brainstem via the vagus nerve
4
,2.3. The gut-brain neural connection
5
, 2.4. PD and α -synuclein pathology in the ENS
Mounting evidence suggests that diseases affecting the CNS could have a
similar pathogenesis in the ENS – one theory holds that insults to the GI
tract may result in α-synuclein pathology in the ENS, which then ascends
along the gut-brain axis to the brain
It is unclear whether α-synuclein pathology begins ‘brain-first’ or ‘gut-first’,
or whether both processes exist within the PD population
The detection of ENS pathology may therefore be potentially useful for the
diagnosis or monitoring of PD, and add to the exciting prospect of
preventing or delaying the onset of PD
2.4.1. PD and α -synuclein pathology in the ENS: evidence from genetic
studies
Genetic risk for PD maps mainly to enteric neurons.
Among all nervous-system cell types analyzed, enteric neurons show
significant enrichment of PD-associated genes.
This suggests that the ENS is a genetically relevant site for PD
pathogenesis, consistent with gut-first models.
Even after adjusting for other neuronal populations, enteric neurons retain
an independent PD genetic signal, indicating a true contribution rather
than spill-over from CNS neurons.
2.5. PD and the gut-brain (or brain-gut) axis
Brain-first = the α-synuclein pathology of PD could begin in the brain and
then spread to the brainstem and the rest of the body
Body-first = the α-synuclein pathology could first arise somewhere in the
body, such as the gut, and then spreads upwards to the brain
6