Anaemia***
08 January 2019 16:53
Micro Normo Macro
Fe ACD Megaloblastic: b12/folate
Non-megaloblastic:
• Alcohol
• Liver failure
• Hypothyroidism
• Myelodysplasia
• Myeloma
• Aplastic anaemia
• Normal in pregnancy and neonates
Thalassaemia /sickle cell Bone marrow failure Reticulocytes - haemolysis
• Malignancy
• Diabetic nephropathy - reduced EPO
Iron deficiency anaemia
• Causes:
a. Reduced iron intake:
▪ Diet -19%
▪ Gastric surgery
▪ Achorhydria
▪ Coeliac disease
b. Blood loss
▪ Unknown origin - 56%
▪ Menstruation
▪ GI
□ Haemorrhoids
□ Peptic ulcers
□ UC
□ Cancer
c. Increased iron requirements
▪ Infancy
▪ Pregnancy
▪ Lactation
d. Unknown - 17%
• C/F:
○ Anaemic symptoms *6
i. Fatigue
ii. Pallor
iii. Chest pain
iv. Palpitations
v. SOB
vi. Dizziness
○ PICA
▪ Craving of non-food substance - ice, dirt, paint
○ Restless leg syndrome
○ Glossitis and angular stomatitis
○ Koilonychias
• IX:
○ Bloods:
▪ FBC
□ Low Hb
□ MCV - microcytic
□ May be Thrombocytosis due to Iron has inhibitory effect on megakaryocytes
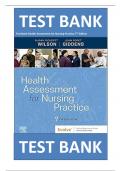
▪ Ferritin - iron storage - diagnostic
□ Also acute phase protein, raised during inflammation
Without iron overload (around 90% of With iron overload (around 10% of patients) - The best test to see whether iron overload
patients) is transferrin saturation.
• Inflammation (due to ferritin being an Primary iron overload (hereditary haemochromatosis)
acute phase reactant)
• Alcohol excess Secondary iron overload (e.g. following repeated transfusions)
• Liver disease
• Chronic kidney disease
• Malignancy
□ If ferritin not reliable:
® Iron studies:
◊ Iron: amount of iron bound to transferrin (buses) - low
◊ Transferrin (buses): more buses needed if low Hb
◊ Transferrin saturation: buses won't be full if low Hb
◊ TIBC/Total Iron binding capacity: the amount of iron transferrin will bind; more free seats if buses are less full
Investigate causes of blood loss:
Haematology Page 1
, ○ Investigate causes of blood loss:
▪ Bedside
□ Urine dipstix
▪ Bloods
□ Ttg-IgA
□ Baseline IgA
▪ Imaging
□ (Urgent) Endoscopy/colonscopy under2 weeks
▪ Special:
□ Blood film --- traget cells
• Rx:
○ 1st line: Oral iron
▪ Ferrous sulphate
□ S/E:
® Dark stools
® Nausea
® Diarrhoea and constipation
▪ Ferrous gluconate/fumirate
○ 2nd line: IV iron
▪ Oral not tolerable or
▪ Rapid loss that oral iron can't keep up
▪ Related to malignancy and IBD
○ If symptomatic/haemodynamically unstable at rest with dyspnoea, chest pain or pre-syncope:
▪ Other forms of replacement still in use: One unit only raise Hb by 1gF/U:
○ Till Hb normal +3months to build up iron storage
Thalassaemia
• Epidemiology:
○ Mediterranean, Middle east, North Africa, India, SE asia
• Aetiology:
○ Autosomal recessive
○ Mutation on Chromosome 11
• Pathophysiology:
○ Quantitative : reduced (intermedia and minor/heterozygous beta thala trait) or absent (major) beta chains --- membrane damage and cell destruction ---
anaemia
○ Ineffective erythropoiesis --- compensatory erythroid hyperplasia/extramedullary haematopoiesis
• C/F:
○ Major
▪ 6months (when HbF (2*alpha + 2*gamma) --- HbA(2*alpha + 2*beta))
▪ Anaemia
□ Pallor
□ Jaundiced - increased haemolysis
□ Poor feeding
□ Failure to thrive
▪ Compensatory mechanisms- erythroid hyperplasia (excessive immature RBC) + extramedullary haematopoiesis:
□ Abdominal distension due to hepatosplenomegaly
□ Bony abnormalities -
® Most often skull:
◊ Large head with Frontal and parietal bossing - flat bones in the cranium
◊ Chipmunk facies - air spaces in the air sinuses
Intermedia:
Haematology Page 2
, ○ Intermedia:
▪ Similar to major but later on as a toddler or older child
▪ Extramedullary haematopoiesis from the vertebral bodies - osteoporotic spine and prone to deformity
○ Minor/beta thala trait:
▪ Usually asymptomatic
▪ Diagnosis based on screening if there's a +ve FH or work up of anaemia (often misdiagnosed is Fe deficiency)
○ Silent carrier:
▪ Completely asymptomatic with normal haematological parameters
• Ix:
○ Bloods:
▪ FBC :
□ microcytic anaemia;
□ elevated leukocyte and platelet counts due to generalised haemtopoietic hyperactivity
□ Disproportionally low MCV comparing to Fe deficiency
▪ Reticulocyte count - elevated as immature RBC
▪ Blood film
▪ LFT - raised unconjugated bilirubin
○ Imaging:
▪ X-ray of skill and long bones
○ Special:
▪ HPLC (high performance liquid chromatography) - diagnostic
□ Type of haemoglobin analysis:
® Raised HbF (2*alpha + 2*gamma) and HbA1 (2*alpha + 2 *delta)
◊ Major: minimal or no HbA
◊ Intermedia: decreased HbA
◊ Minor/trait: mostly HbA
• Rx:
○ Minor/trait :
▪ Conservative:
□ Asymptomatic, normally no treatment required
□ Genetic counselling
○ Intermedia :
▪ Non-transfusion dependant - moderate anaemia:
□ Conservative:
® Genetic counselling
□ Medical:
® Only transfuse if anaemic during stress: e.g. infection
® Only splenectomy if massively enlarged
® Iron monitoring and chelating therapy:
◊ Even if not transfused, increased absorption of iron from the gut driven by ineffective erythropoiesis,cumulative process, occur much
later in life than transfusion dependant
▪ Transfusion dependant due to profound anaemia, symptomatic, impaired growth and development:
□ Conservative:
® Genetic counselling
□ Medical:
® Regular transfusions:
◊ S/E: iron overload:
} Deposition in heart/pancreas
} Monitor LIC (liver iron concentration), myocardial T2 & pancreatic MRI
} Iron chelating therapy - de-ferrioxamine
□ Surgical:
® Splenectomy:
◊ Inevitable due to extramedullary haematopoisis - hypersplenism - destruction of red cells -- profound anaemia
◊ Hyposplenism post splenectomy:
} Prone to encapsulated infections,
– Abx prophylaxis - penicillin V or amoxicillin daily
– Vaccination (MenC, Men ACWY, Hib, pneumococcal, annual influenza )
} Risk of VTE and pulmonary hypertension
® Stem cell transplant - curative
○ Major:
▪ As per Transfusion dependant intermedia
• Complications:
○ Iron overload:
▪ Endocrinological:
□ Anterior pituitary:
® GH: slowed growth
® Delayed sexual maturation, infertility (may be due to direct iron deposition in the gonads)
□ Pancreas:
® Impaired insulin secretion and abnormal glucose tolerance --- Type 1 DM
□ Parathyroid:
® Osteopenia/osteoporosis
▪ Skin - pigmentation/bronzing
▪ Heart - heart failure
○ Transfusion related reactions
▪ Immunological
□ Acute haemolytic
□ Non-haemolytic febrile
Haematology Page 3
, □ Non-haemolytic febrile
□ Allergic/anaphylactic
▪ infective
○ Thrombosis
Sickle cell
• Definition:
○ Autosomal recessive
▪ Sickle trait: sickle gene from one parent and normal from another
▪ Sickle disease: sickle from both parents
▪ Sickle beta-thalassaemia: HbS (one parent) and beta-thalassaemia (another parent)
○ Qualitative: defect in beta chain in HbA to form HbS
• Epidemiology:
○ Black populations; carrier protective against severe malaria
• Aetiology:
○ Haemoglobin becomes rigid and distorted into crescent shape,
○ very fragile, easier to haemolyse and blocking small vessels to cause infarction
• Pathophysiology:
○ Triggers of sickling:
i. Cold temperature
ii. Infection
iii. Hypoxia
iv. Acidosis
v. Extreme exercise
vi. Dehydration
• C/F:
○ Haemolytic anaemia
▪ Pallor
▪ Jaundice
▪ Poor feeding
▪ Cardiomegaly
○ Vaso-occlusive/ thrombotic painful crisis:
▪ Stroke
▪ Visual floaters:
□ Occlusions in retinal arterioles leading to neovascualrisation - haemorrhage - retinal detachment
▪ ACS (acute chest syndrome)
□ Clinically indistinguishable from pneumonia
□ SOB, cough
□ T-shirt pain distribution
□ CXR: bilateral pulmonary infiltrates
▪ Spleen
□ Sequestration (holding off and pooling of RBC - worsening anaemia but with raised reticulocyte count, could potentially be life-threatening)
® Circulatory failure
□ Infarction
▪ Priapism (unwanted erections)
▪ Joints:
□ Bone pain due to AVN - osteolytic destruction with overlying periosteal new bone formation
□ Swelling of hands &feet/dactylitis --- often the 1st presenting symptom- stops at 5 y/o as no more haematopoiesis in small bones
Haematology Page 4
08 January 2019 16:53
Micro Normo Macro
Fe ACD Megaloblastic: b12/folate
Non-megaloblastic:
• Alcohol
• Liver failure
• Hypothyroidism
• Myelodysplasia
• Myeloma
• Aplastic anaemia
• Normal in pregnancy and neonates
Thalassaemia /sickle cell Bone marrow failure Reticulocytes - haemolysis
• Malignancy
• Diabetic nephropathy - reduced EPO
Iron deficiency anaemia
• Causes:
a. Reduced iron intake:
▪ Diet -19%
▪ Gastric surgery
▪ Achorhydria
▪ Coeliac disease
b. Blood loss
▪ Unknown origin - 56%
▪ Menstruation
▪ GI
□ Haemorrhoids
□ Peptic ulcers
□ UC
□ Cancer
c. Increased iron requirements
▪ Infancy
▪ Pregnancy
▪ Lactation
d. Unknown - 17%
• C/F:
○ Anaemic symptoms *6
i. Fatigue
ii. Pallor
iii. Chest pain
iv. Palpitations
v. SOB
vi. Dizziness
○ PICA
▪ Craving of non-food substance - ice, dirt, paint
○ Restless leg syndrome
○ Glossitis and angular stomatitis
○ Koilonychias
• IX:
○ Bloods:
▪ FBC
□ Low Hb
□ MCV - microcytic
□ May be Thrombocytosis due to Iron has inhibitory effect on megakaryocytes
▪ Ferritin - iron storage - diagnostic
□ Also acute phase protein, raised during inflammation
Without iron overload (around 90% of With iron overload (around 10% of patients) - The best test to see whether iron overload
patients) is transferrin saturation.
• Inflammation (due to ferritin being an Primary iron overload (hereditary haemochromatosis)
acute phase reactant)
• Alcohol excess Secondary iron overload (e.g. following repeated transfusions)
• Liver disease
• Chronic kidney disease
• Malignancy
□ If ferritin not reliable:
® Iron studies:
◊ Iron: amount of iron bound to transferrin (buses) - low
◊ Transferrin (buses): more buses needed if low Hb
◊ Transferrin saturation: buses won't be full if low Hb
◊ TIBC/Total Iron binding capacity: the amount of iron transferrin will bind; more free seats if buses are less full
Investigate causes of blood loss:
Haematology Page 1
, ○ Investigate causes of blood loss:
▪ Bedside
□ Urine dipstix
▪ Bloods
□ Ttg-IgA
□ Baseline IgA
▪ Imaging
□ (Urgent) Endoscopy/colonscopy under2 weeks
▪ Special:
□ Blood film --- traget cells
• Rx:
○ 1st line: Oral iron
▪ Ferrous sulphate
□ S/E:
® Dark stools
® Nausea
® Diarrhoea and constipation
▪ Ferrous gluconate/fumirate
○ 2nd line: IV iron
▪ Oral not tolerable or
▪ Rapid loss that oral iron can't keep up
▪ Related to malignancy and IBD
○ If symptomatic/haemodynamically unstable at rest with dyspnoea, chest pain or pre-syncope:
▪ Other forms of replacement still in use: One unit only raise Hb by 1gF/U:
○ Till Hb normal +3months to build up iron storage
Thalassaemia
• Epidemiology:
○ Mediterranean, Middle east, North Africa, India, SE asia
• Aetiology:
○ Autosomal recessive
○ Mutation on Chromosome 11
• Pathophysiology:
○ Quantitative : reduced (intermedia and minor/heterozygous beta thala trait) or absent (major) beta chains --- membrane damage and cell destruction ---
anaemia
○ Ineffective erythropoiesis --- compensatory erythroid hyperplasia/extramedullary haematopoiesis
• C/F:
○ Major
▪ 6months (when HbF (2*alpha + 2*gamma) --- HbA(2*alpha + 2*beta))
▪ Anaemia
□ Pallor
□ Jaundiced - increased haemolysis
□ Poor feeding
□ Failure to thrive
▪ Compensatory mechanisms- erythroid hyperplasia (excessive immature RBC) + extramedullary haematopoiesis:
□ Abdominal distension due to hepatosplenomegaly
□ Bony abnormalities -
® Most often skull:
◊ Large head with Frontal and parietal bossing - flat bones in the cranium
◊ Chipmunk facies - air spaces in the air sinuses
Intermedia:
Haematology Page 2
, ○ Intermedia:
▪ Similar to major but later on as a toddler or older child
▪ Extramedullary haematopoiesis from the vertebral bodies - osteoporotic spine and prone to deformity
○ Minor/beta thala trait:
▪ Usually asymptomatic
▪ Diagnosis based on screening if there's a +ve FH or work up of anaemia (often misdiagnosed is Fe deficiency)
○ Silent carrier:
▪ Completely asymptomatic with normal haematological parameters
• Ix:
○ Bloods:
▪ FBC :
□ microcytic anaemia;
□ elevated leukocyte and platelet counts due to generalised haemtopoietic hyperactivity
□ Disproportionally low MCV comparing to Fe deficiency
▪ Reticulocyte count - elevated as immature RBC
▪ Blood film
▪ LFT - raised unconjugated bilirubin
○ Imaging:
▪ X-ray of skill and long bones
○ Special:
▪ HPLC (high performance liquid chromatography) - diagnostic
□ Type of haemoglobin analysis:
® Raised HbF (2*alpha + 2*gamma) and HbA1 (2*alpha + 2 *delta)
◊ Major: minimal or no HbA
◊ Intermedia: decreased HbA
◊ Minor/trait: mostly HbA
• Rx:
○ Minor/trait :
▪ Conservative:
□ Asymptomatic, normally no treatment required
□ Genetic counselling
○ Intermedia :
▪ Non-transfusion dependant - moderate anaemia:
□ Conservative:
® Genetic counselling
□ Medical:
® Only transfuse if anaemic during stress: e.g. infection
® Only splenectomy if massively enlarged
® Iron monitoring and chelating therapy:
◊ Even if not transfused, increased absorption of iron from the gut driven by ineffective erythropoiesis,cumulative process, occur much
later in life than transfusion dependant
▪ Transfusion dependant due to profound anaemia, symptomatic, impaired growth and development:
□ Conservative:
® Genetic counselling
□ Medical:
® Regular transfusions:
◊ S/E: iron overload:
} Deposition in heart/pancreas
} Monitor LIC (liver iron concentration), myocardial T2 & pancreatic MRI
} Iron chelating therapy - de-ferrioxamine
□ Surgical:
® Splenectomy:
◊ Inevitable due to extramedullary haematopoisis - hypersplenism - destruction of red cells -- profound anaemia
◊ Hyposplenism post splenectomy:
} Prone to encapsulated infections,
– Abx prophylaxis - penicillin V or amoxicillin daily
– Vaccination (MenC, Men ACWY, Hib, pneumococcal, annual influenza )
} Risk of VTE and pulmonary hypertension
® Stem cell transplant - curative
○ Major:
▪ As per Transfusion dependant intermedia
• Complications:
○ Iron overload:
▪ Endocrinological:
□ Anterior pituitary:
® GH: slowed growth
® Delayed sexual maturation, infertility (may be due to direct iron deposition in the gonads)
□ Pancreas:
® Impaired insulin secretion and abnormal glucose tolerance --- Type 1 DM
□ Parathyroid:
® Osteopenia/osteoporosis
▪ Skin - pigmentation/bronzing
▪ Heart - heart failure
○ Transfusion related reactions
▪ Immunological
□ Acute haemolytic
□ Non-haemolytic febrile
Haematology Page 3
, □ Non-haemolytic febrile
□ Allergic/anaphylactic
▪ infective
○ Thrombosis
Sickle cell
• Definition:
○ Autosomal recessive
▪ Sickle trait: sickle gene from one parent and normal from another
▪ Sickle disease: sickle from both parents
▪ Sickle beta-thalassaemia: HbS (one parent) and beta-thalassaemia (another parent)
○ Qualitative: defect in beta chain in HbA to form HbS
• Epidemiology:
○ Black populations; carrier protective against severe malaria
• Aetiology:
○ Haemoglobin becomes rigid and distorted into crescent shape,
○ very fragile, easier to haemolyse and blocking small vessels to cause infarction
• Pathophysiology:
○ Triggers of sickling:
i. Cold temperature
ii. Infection
iii. Hypoxia
iv. Acidosis
v. Extreme exercise
vi. Dehydration
• C/F:
○ Haemolytic anaemia
▪ Pallor
▪ Jaundice
▪ Poor feeding
▪ Cardiomegaly
○ Vaso-occlusive/ thrombotic painful crisis:
▪ Stroke
▪ Visual floaters:
□ Occlusions in retinal arterioles leading to neovascualrisation - haemorrhage - retinal detachment
▪ ACS (acute chest syndrome)
□ Clinically indistinguishable from pneumonia
□ SOB, cough
□ T-shirt pain distribution
□ CXR: bilateral pulmonary infiltrates
▪ Spleen
□ Sequestration (holding off and pooling of RBC - worsening anaemia but with raised reticulocyte count, could potentially be life-threatening)
® Circulatory failure
□ Infarction
▪ Priapism (unwanted erections)
▪ Joints:
□ Bone pain due to AVN - osteolytic destruction with overlying periosteal new bone formation
□ Swelling of hands &feet/dactylitis --- often the 1st presenting symptom- stops at 5 y/o as no more haematopoiesis in small bones
Haematology Page 4