Cognitive psychology II
Chapters
GUEST LECTURE: Parkinson’s disease .......................................................................................................................................... 1
GUEST LECTURE: Mindfulness and Cognition ....................................................................................................................... 36
GUEST LECTURE: Eating Disorders ............................................................................................................................................. 56
GUEST LECTURE: Social Cognition and ASD .......................................................................................................................... 73
GUEST LECTURE: Unilateral neglect following brain damage ......................................................................................... 85
GUEST LECTURE: Sleep Disorders and Cognition .............................................................................................................. 106
Algemene competenties
1. The student will acquire advanced knowledge about human cognition.
2. The student will obtain a deeper understanding of the interaction between theory and
research in cognitive (neuro)psychology.
3. The student can independently engage in scientific reasoning, and critically evaluate new
scientific findings.
Gastcolleges (6)
English Multiple Choice Exam
,GUEST LECTURE: PARKINSON’S DISEASE
Theoretical background
Parkinson’s disease (PD)
Chronic Progressive Degenerative Brain Disorder
‘chronic’ ⇛ persistent disease, can’t be cured as of yet
‘progressive’ ⇛ symptoms worsen over time
‘degenerative’ ⇛ disease is result of a continuous process based on degenerative cell changes,
which will increasingly deteriorate over time
↬ Fastest growing neurological disorder
# People with PD ⇛ doubled with 6 million over last 3 decades
⇛ will double again with over 12 million by 2040
↬ Second-most common neurodegenerative disorder
2-3% of population ≥65 years of age
↬ Cause: degeneration of dopamine-producing cells in the
substantia nigra of the basal ganglia
Dopamine = neurotransmitter ⇛ loss of dopamine in people with PD causes cascade of
activity changes in brain, which manifest in the following effects:
↬ Effect:
Typical motor symptoms: resting tremor, general slowness of movements, rigidity & postural
instability
Non-motor features: cognitive deficits
Neurobehavioral abnormalities:
Epidemiology
↬ Estimated global incidence: 5 to 230 new cases per 100,000 individuals yearly. Rare before age 50
↬ Incidence 5 to 10-fold from ages 60-90
↬ Global prevalence estimated 0.3%
Increases to >3% in >80 years
↬ Usually: onset between ages 60-70
↬ Genetic variant: Young Onset PD (occurs in younger adults)
5-20% of persons w/ PD
1|Page
,↬ Generally speaking, mortality is not increased in first 10 years after disease onset, but it does
increase afterwards, sometimes eventually even doubling compared to general population
Male: Female distribution ± 1.5:1
↬ Almost twice as common in ♂ than in ♀ in most populations
↬ Females sex hormones, genetic mechanisms, or sex specific differences in exposure to
environmental risk factors may explain why ♂ are most likely to get PD
Etiology
↬ Most cases: idiopathic (no known cause)
↬ Most likely a combination of factors:
Age
⤷ largest risk factor for developing PD; not very clear how it works
Environmental (toxins, pesiticides, insecticides: rotenone, paraquat, MPTP)
ex. MPTP = toxin: organic compound which induces toxic effects on substantia nigra
(regulation of motor skills) ⇾ MPTP toxin gives Parkinson’s like symptoms: kind of mimics
pathophysiological mechanism which causes PD
Dietary (pollutants)
Genetic predisposition (mutations in ⍺-synuclein, LRRK2, GBA) e.g. Ashkenazi Jews (Israel), Inuit (Alaska)
⤷ genetics cause 10-15% of PD
⤷ in some families changes in mutations in certain genes are inherited from generation to
generation
⤷ some ethnical groups more commonly carry genes linked to PD (see e.g. above) ex. LRRK2
Brain trauma, stroke, viral inflammation
⤷ even years after injury
Both environmental & genetic factors contribute to onset of illness (age remains main factor)
Oxidative stress destroys mitochondria ⇛ apoptosis (cell death) of dopaminergic cells.
⤷ cigarette smoking & caffeine may decrease risk ⇛ mostly due to protective factor of nicotine &
caffeine
2|Page
, Pathophysiology
Characteristic features:
1. Loss of dopaminergic neurons in the pars compacta of the substantia nigra
NO general macroscopic atrophy (shrinking) of the brain, but degeneration in certain types of
neurons within particular brain regions.
E.g. early-stage PD: loss of dopaminergic neurons restricted to VL substantia nigra
⤷ suggest that degeneration in this region starts before onset of motor symptoms
end-stage PD: more widespread loss
Resulting in a reduction of the neurotransmitter dopamine in the basal ganglia
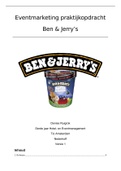
Panels A and B represent the human postmortem bilateral midbrain of normal and
Parkinsonian subjects, respectively.
Much less pronounced dark area with dopaminergic cells in substantia nigra in B than in A
2. Widespread protein (⍺-synuclein) accumulation (“Lewy Bodies”) in neurons
Proteins accumulate in substantia nigra & form clusters = “Lewy Bodies”
The Basal Ganglia: Aantomy
5 interconnected sub-cortical nuclei:
3|Page
Chapters
GUEST LECTURE: Parkinson’s disease .......................................................................................................................................... 1
GUEST LECTURE: Mindfulness and Cognition ....................................................................................................................... 36
GUEST LECTURE: Eating Disorders ............................................................................................................................................. 56
GUEST LECTURE: Social Cognition and ASD .......................................................................................................................... 73
GUEST LECTURE: Unilateral neglect following brain damage ......................................................................................... 85
GUEST LECTURE: Sleep Disorders and Cognition .............................................................................................................. 106
Algemene competenties
1. The student will acquire advanced knowledge about human cognition.
2. The student will obtain a deeper understanding of the interaction between theory and
research in cognitive (neuro)psychology.
3. The student can independently engage in scientific reasoning, and critically evaluate new
scientific findings.
Gastcolleges (6)
English Multiple Choice Exam
,GUEST LECTURE: PARKINSON’S DISEASE
Theoretical background
Parkinson’s disease (PD)
Chronic Progressive Degenerative Brain Disorder
‘chronic’ ⇛ persistent disease, can’t be cured as of yet
‘progressive’ ⇛ symptoms worsen over time
‘degenerative’ ⇛ disease is result of a continuous process based on degenerative cell changes,
which will increasingly deteriorate over time
↬ Fastest growing neurological disorder
# People with PD ⇛ doubled with 6 million over last 3 decades
⇛ will double again with over 12 million by 2040
↬ Second-most common neurodegenerative disorder
2-3% of population ≥65 years of age
↬ Cause: degeneration of dopamine-producing cells in the
substantia nigra of the basal ganglia
Dopamine = neurotransmitter ⇛ loss of dopamine in people with PD causes cascade of
activity changes in brain, which manifest in the following effects:
↬ Effect:
Typical motor symptoms: resting tremor, general slowness of movements, rigidity & postural
instability
Non-motor features: cognitive deficits
Neurobehavioral abnormalities:
Epidemiology
↬ Estimated global incidence: 5 to 230 new cases per 100,000 individuals yearly. Rare before age 50
↬ Incidence 5 to 10-fold from ages 60-90
↬ Global prevalence estimated 0.3%
Increases to >3% in >80 years
↬ Usually: onset between ages 60-70
↬ Genetic variant: Young Onset PD (occurs in younger adults)
5-20% of persons w/ PD
1|Page
,↬ Generally speaking, mortality is not increased in first 10 years after disease onset, but it does
increase afterwards, sometimes eventually even doubling compared to general population
Male: Female distribution ± 1.5:1
↬ Almost twice as common in ♂ than in ♀ in most populations
↬ Females sex hormones, genetic mechanisms, or sex specific differences in exposure to
environmental risk factors may explain why ♂ are most likely to get PD
Etiology
↬ Most cases: idiopathic (no known cause)
↬ Most likely a combination of factors:
Age
⤷ largest risk factor for developing PD; not very clear how it works
Environmental (toxins, pesiticides, insecticides: rotenone, paraquat, MPTP)
ex. MPTP = toxin: organic compound which induces toxic effects on substantia nigra
(regulation of motor skills) ⇾ MPTP toxin gives Parkinson’s like symptoms: kind of mimics
pathophysiological mechanism which causes PD
Dietary (pollutants)
Genetic predisposition (mutations in ⍺-synuclein, LRRK2, GBA) e.g. Ashkenazi Jews (Israel), Inuit (Alaska)
⤷ genetics cause 10-15% of PD
⤷ in some families changes in mutations in certain genes are inherited from generation to
generation
⤷ some ethnical groups more commonly carry genes linked to PD (see e.g. above) ex. LRRK2
Brain trauma, stroke, viral inflammation
⤷ even years after injury
Both environmental & genetic factors contribute to onset of illness (age remains main factor)
Oxidative stress destroys mitochondria ⇛ apoptosis (cell death) of dopaminergic cells.
⤷ cigarette smoking & caffeine may decrease risk ⇛ mostly due to protective factor of nicotine &
caffeine
2|Page
, Pathophysiology
Characteristic features:
1. Loss of dopaminergic neurons in the pars compacta of the substantia nigra
NO general macroscopic atrophy (shrinking) of the brain, but degeneration in certain types of
neurons within particular brain regions.
E.g. early-stage PD: loss of dopaminergic neurons restricted to VL substantia nigra
⤷ suggest that degeneration in this region starts before onset of motor symptoms
end-stage PD: more widespread loss
Resulting in a reduction of the neurotransmitter dopamine in the basal ganglia
Panels A and B represent the human postmortem bilateral midbrain of normal and
Parkinsonian subjects, respectively.
Much less pronounced dark area with dopaminergic cells in substantia nigra in B than in A
2. Widespread protein (⍺-synuclein) accumulation (“Lewy Bodies”) in neurons
Proteins accumulate in substantia nigra & form clusters = “Lewy Bodies”
The Basal Ganglia: Aantomy
5 interconnected sub-cortical nuclei:
3|Page