PRAKTIJK OL — ESSENTIE
Klinisch onderzoek heup
Neurologisch
Art. Coxae bezenuwd door: n. femorlis (anterieur), plexus sacralis (posterieur), n
obturatorius (mediaal)
Inspectie
Na te gaan of de afwijking sturctureel of functioneel is, op basis van de musculatuur
Spiertrofiek link-rechts vergelijken
Hoek tussen collum femoris en schaft: optimale krachtvecto is in het midden van
acetabulum
- Normaal = 125°
- Coxa valga = 140° = varus stand in de knie (O-benen) (krachtvector te hoog)
- Coxa vara = 105° = valgus stand in de knie (X-benen) (krachtvector te laag)
Ante-/retroversie: Craige’s test (niet zo betrouwbaar)
- Normaal = 15°
- Anteversie = 35° = meer druk anterieure labrium = voeten naar binnen (te grote
hoek)
- Retroversie = 5° = meer druk posterieure labrium = voeten naar buiten (te kleine
hoek)
Palpatie
Voor en na KO = Temperatuur + zwelling
Einde van het KO = structuurpalpatie = provocatie!
Actief bewegelijkheidsonderzoek
Functioneel
Keuze van test afhankelijk van anamnese
- Afwijkingen/problemen thv knie en/of enkel en voet kunnen ook gevolgen hebben
thv heup!
- Bv; trap afgaan, auto instappen, springen, etc.
Lokaal-anatomische test
Eerst niet aangedane zijde testen
- Endorotatie/exorotatie (knie en heup 90° gebogen)
- Extensie (P in voorlig)
- Flexie
- Adductie/abductie
Passief bewegelijkheidsonderzoek
Rol & glij tegensgesteld: Caput femoris = convex/Fossa acetabuli = concaaf
1
,Doel: ROM + pijn + trajectweerstand + eindgevoel = elastisch
Bewegin Spier Innervatie Segmenten
g
Flexie M. iliopsoas Plexus lumbalis L2–L4
M. sartorius N. femoralis L2–L4
M. rectus femoris N. femoralis L2–L4
M. pectineus N. femoralis / N. obturatori L2–L4
M. adductor longus us L2–L4
M. tensor fasciae latae N. obturatorius L4–S1
M. adductor brevis N. gluteus superior L2–L4
N. obturatorius
Extensie M. gluteus maximus N. gluteus inferior L5–S2
M. semitendinosus N. ischiadicus L4–S2(3)
M. semimembranosus N. ischiadicus L4–S2(3)
M. biceps femoris, caput lon N. ischiadicus L4–S2(3)
gum N. peroneus communis L4–S2
M. biceps femoris, caput bre N. obturatorius / N. ischiad L2–L4 / L4–
ve icus S2(3)
M. adductor magnus
Adductie M. pectineus N. femoralis / N. obturatori L2–L4
M. adductor longus us L2–L4
M. adductor brevis N. obturatorius L2–L4
M. adductor magnus N. obturatorius L2–L4 / L4–
M. gracilis N. obturatorius / N. ischiad S2(3)
M. quadratus femoris icus L2–L4
M. obturatorius externus N. obturatorius L4–S1
Plexus sacralis L2–L4
N. obturatorius
Abductie M. gluteus medius N. gluteus superior L4–S1
M. gluteus minimus N. gluteus superior L4–S1
M. tensor fasciae latae N. gluteus superior L4–S1
M. piriformis Plexus sacralis S1–S1
M. sartorius N. femoralis L2–L4
M. obturatorius internus Plexus sacralis L5–S2
Mm. gemelli Plexus sacralis L4–S2
Exorotati M. gluteus maximus N. gluteus inferior L5–S2
e M. quadratus femoris Plexus sacralis L4–S1
M. obturatorius internus Plexus sacralis L5–S2
Mm. gemelli Plexus sacralis L4–S2
M. iliopsoas Plexus lumbalis L2–L4
M. sartorius N. femoralis L2–L4
M. gluteus medius (pars post N. gluteus superior L4–S1
2
, erior) Plexus sacralis S1–S2
M. piriformis N. obturatorius L2–L4
M. obturatorius externus
Endorota M. gluteus minimus N. gluteus superior L4–S1
tie M. gluteus medius (pars ante N. gluteus superior L4–S1
rior) N. gluteus superior L4–S1
M. tensor fasciae latae
3
, Neuromusculair onderzoek
6 belangrijke puntjes
1. Kracht
2. Uithouding
3. Pijn (bevragen)
4. Proprioceptie
5. Coördinatie
6. Positie- en bewegingszin
Drie grote groepen testen
1. Isometrische krachttesten
2. Spierlengtetesten
3. Dynamische spierwerking
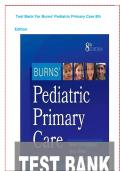
Neuromusculair onderzoek dissociatietest abductie
Patiënt stabiliseert het bekken en voert een abductie uit met het bovenliggende been.
Normaal gebeurt er een zuivere abductie (M. Gluteus Medius dominant), maar bij een
dominantie van tensor fasciae latae zal de heup in flexie (been komt naar voor) en/of
endorotatie (tenen naar beneden) bewegen.
4
, Neuromusculair onderzoek dissociatietest abductie-exorotatie
Patiënt stabiliseert romp en bekken, houdt voeten op elkaar en draait bovenliggende knie
naar boven. Normaal wordt deze beweging uitgevoerd met de exorotatoren en
posterieure deel van gluteus medius. Bij problemen zal deze beweging eerder uitgevoerd
worden met behulp van tensor fasciae latae.
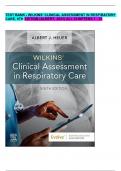
Neuromusculair onderzoek dissociatietest extensie met knieflexie
Been in omgekeerd 4 teken (30° ABductie heup). De patiënt dient gluteus maximus
geïsoleerd aan te spannen zonder contractie van hamstrings
5
Klinisch onderzoek heup
Neurologisch
Art. Coxae bezenuwd door: n. femorlis (anterieur), plexus sacralis (posterieur), n
obturatorius (mediaal)
Inspectie
Na te gaan of de afwijking sturctureel of functioneel is, op basis van de musculatuur
Spiertrofiek link-rechts vergelijken
Hoek tussen collum femoris en schaft: optimale krachtvecto is in het midden van
acetabulum
- Normaal = 125°
- Coxa valga = 140° = varus stand in de knie (O-benen) (krachtvector te hoog)
- Coxa vara = 105° = valgus stand in de knie (X-benen) (krachtvector te laag)
Ante-/retroversie: Craige’s test (niet zo betrouwbaar)
- Normaal = 15°
- Anteversie = 35° = meer druk anterieure labrium = voeten naar binnen (te grote
hoek)
- Retroversie = 5° = meer druk posterieure labrium = voeten naar buiten (te kleine
hoek)
Palpatie
Voor en na KO = Temperatuur + zwelling
Einde van het KO = structuurpalpatie = provocatie!
Actief bewegelijkheidsonderzoek
Functioneel
Keuze van test afhankelijk van anamnese
- Afwijkingen/problemen thv knie en/of enkel en voet kunnen ook gevolgen hebben
thv heup!
- Bv; trap afgaan, auto instappen, springen, etc.
Lokaal-anatomische test
Eerst niet aangedane zijde testen
- Endorotatie/exorotatie (knie en heup 90° gebogen)
- Extensie (P in voorlig)
- Flexie
- Adductie/abductie
Passief bewegelijkheidsonderzoek
Rol & glij tegensgesteld: Caput femoris = convex/Fossa acetabuli = concaaf
1
,Doel: ROM + pijn + trajectweerstand + eindgevoel = elastisch
Bewegin Spier Innervatie Segmenten
g
Flexie M. iliopsoas Plexus lumbalis L2–L4
M. sartorius N. femoralis L2–L4
M. rectus femoris N. femoralis L2–L4
M. pectineus N. femoralis / N. obturatori L2–L4
M. adductor longus us L2–L4
M. tensor fasciae latae N. obturatorius L4–S1
M. adductor brevis N. gluteus superior L2–L4
N. obturatorius
Extensie M. gluteus maximus N. gluteus inferior L5–S2
M. semitendinosus N. ischiadicus L4–S2(3)
M. semimembranosus N. ischiadicus L4–S2(3)
M. biceps femoris, caput lon N. ischiadicus L4–S2(3)
gum N. peroneus communis L4–S2
M. biceps femoris, caput bre N. obturatorius / N. ischiad L2–L4 / L4–
ve icus S2(3)
M. adductor magnus
Adductie M. pectineus N. femoralis / N. obturatori L2–L4
M. adductor longus us L2–L4
M. adductor brevis N. obturatorius L2–L4
M. adductor magnus N. obturatorius L2–L4 / L4–
M. gracilis N. obturatorius / N. ischiad S2(3)
M. quadratus femoris icus L2–L4
M. obturatorius externus N. obturatorius L4–S1
Plexus sacralis L2–L4
N. obturatorius
Abductie M. gluteus medius N. gluteus superior L4–S1
M. gluteus minimus N. gluteus superior L4–S1
M. tensor fasciae latae N. gluteus superior L4–S1
M. piriformis Plexus sacralis S1–S1
M. sartorius N. femoralis L2–L4
M. obturatorius internus Plexus sacralis L5–S2
Mm. gemelli Plexus sacralis L4–S2
Exorotati M. gluteus maximus N. gluteus inferior L5–S2
e M. quadratus femoris Plexus sacralis L4–S1
M. obturatorius internus Plexus sacralis L5–S2
Mm. gemelli Plexus sacralis L4–S2
M. iliopsoas Plexus lumbalis L2–L4
M. sartorius N. femoralis L2–L4
M. gluteus medius (pars post N. gluteus superior L4–S1
2
, erior) Plexus sacralis S1–S2
M. piriformis N. obturatorius L2–L4
M. obturatorius externus
Endorota M. gluteus minimus N. gluteus superior L4–S1
tie M. gluteus medius (pars ante N. gluteus superior L4–S1
rior) N. gluteus superior L4–S1
M. tensor fasciae latae
3
, Neuromusculair onderzoek
6 belangrijke puntjes
1. Kracht
2. Uithouding
3. Pijn (bevragen)
4. Proprioceptie
5. Coördinatie
6. Positie- en bewegingszin
Drie grote groepen testen
1. Isometrische krachttesten
2. Spierlengtetesten
3. Dynamische spierwerking
Neuromusculair onderzoek dissociatietest abductie
Patiënt stabiliseert het bekken en voert een abductie uit met het bovenliggende been.
Normaal gebeurt er een zuivere abductie (M. Gluteus Medius dominant), maar bij een
dominantie van tensor fasciae latae zal de heup in flexie (been komt naar voor) en/of
endorotatie (tenen naar beneden) bewegen.
4
, Neuromusculair onderzoek dissociatietest abductie-exorotatie
Patiënt stabiliseert romp en bekken, houdt voeten op elkaar en draait bovenliggende knie
naar boven. Normaal wordt deze beweging uitgevoerd met de exorotatoren en
posterieure deel van gluteus medius. Bij problemen zal deze beweging eerder uitgevoerd
worden met behulp van tensor fasciae latae.
Neuromusculair onderzoek dissociatietest extensie met knieflexie
Been in omgekeerd 4 teken (30° ABductie heup). De patiënt dient gluteus maximus
geïsoleerd aan te spannen zonder contractie van hamstrings
5