EDPNA Exam – ESRD Dietitian
Preceptor/Preceptor Nursing Assessment
Certification Practice
Save
Practice questions for this set
Learn 1 /7 Study using Learn
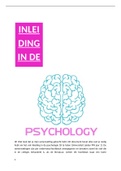
*Increase in Serum Creatinine &
*Decreased Urine Output
Choose an answer
Nephrotic Syndrome? Caused by?
1 2 Acute Kidney Injury Staging
Leads to?
Protein requirement g/kg CKD
3 Unstable patient criteria 4
(stages 3-5)
Don't know?
, Terms in this set (78)
Glomerular damage (from lupus, autoimmune dx, DM,
Nephrotic Syndrome?
toxins, collagen vascular dx)
Caused by? Leads to?
Leads to proteinuria
(>3g/day SHOULD BE less than 150mg)
fatigued
Proteinuria g/day, s/s ineffective healing
lose muscle mass
3rd spacing (ascites, edema)
*Sodium: 2g restriction
Nephrotic Syndrome Tx: *Fluid restriction ONLY if RF
sodium, fluid, protein, *Protein: DONT PUT ON HIGH PROTEIN-only 24hr
calories, Deficiency urine collection loss+RDA ( 0.7-0.8 g protein/kg)
repletion *Calories for healing
*Replete Vit D, Ca, bicarb, iron deficiencies
Protein requirement g/kg 0.8 g/kg
RDA
Protein requirement g/kg Non-DM 0.55-0.6 g/kg
CKD (stages 3-5) DM 0.6-0.8 g/kg
Protein requirement g/kg Non-DM or DM 1.0-1.2 g/kg
CKD (stage 5D: HD/PD)
CKD (all stages & dialysis) 25-35 Kcal/kg
Energy Kcal/kg
-Adjust dietary Phos intake to maintain serum P levels
Phosphorus mg/day CKD -Consider bioavailability of Phos sources
(all stages) -Posttransplant or Low Phos, Rx high phos diet and/or
suppl
Potassium mEq/d CKD (all Maintain normal serum range with diet and suppl prn
stages and post
transplant)
Preceptor/Preceptor Nursing Assessment
Certification Practice
Save
Practice questions for this set
Learn 1 /7 Study using Learn
*Increase in Serum Creatinine &
*Decreased Urine Output
Choose an answer
Nephrotic Syndrome? Caused by?
1 2 Acute Kidney Injury Staging
Leads to?
Protein requirement g/kg CKD
3 Unstable patient criteria 4
(stages 3-5)
Don't know?
, Terms in this set (78)
Glomerular damage (from lupus, autoimmune dx, DM,
Nephrotic Syndrome?
toxins, collagen vascular dx)
Caused by? Leads to?
Leads to proteinuria
(>3g/day SHOULD BE less than 150mg)
fatigued
Proteinuria g/day, s/s ineffective healing
lose muscle mass
3rd spacing (ascites, edema)
*Sodium: 2g restriction
Nephrotic Syndrome Tx: *Fluid restriction ONLY if RF
sodium, fluid, protein, *Protein: DONT PUT ON HIGH PROTEIN-only 24hr
calories, Deficiency urine collection loss+RDA ( 0.7-0.8 g protein/kg)
repletion *Calories for healing
*Replete Vit D, Ca, bicarb, iron deficiencies
Protein requirement g/kg 0.8 g/kg
RDA
Protein requirement g/kg Non-DM 0.55-0.6 g/kg
CKD (stages 3-5) DM 0.6-0.8 g/kg
Protein requirement g/kg Non-DM or DM 1.0-1.2 g/kg
CKD (stage 5D: HD/PD)
CKD (all stages & dialysis) 25-35 Kcal/kg
Energy Kcal/kg
-Adjust dietary Phos intake to maintain serum P levels
Phosphorus mg/day CKD -Consider bioavailability of Phos sources
(all stages) -Posttransplant or Low Phos, Rx high phos diet and/or
suppl
Potassium mEq/d CKD (all Maintain normal serum range with diet and suppl prn
stages and post
transplant)