Clinical Anatomy 32:156–163 (2019)
MEDICAL AND DENTAL EDUCATION
An Evidence-Based Approach to Learning
Clinical Anatomy: A Guide for Medical Students,
Educators, and Administrators
ANTHONY V. D’ANTONI ,1* ESTOMIH P. MTUI,1 MARIOS LOUKAS ,2
R. SHANE TUBBS ,3 GENEVIEVE PINTO ZIPP,4 AND JOHN DUNLOSKY5
1
Division of Anatomy, Department of Radiology, Weill Cornell Medicine, New York, New York
2
Department of Anatomical Sciences, St. George’s University School of Medicine, Grenada, West Indies
3
Seattle Science Foundation, Seattle, Washington
4
Department of Interprofessional Health Sciences and Health Administration, School of Health and
Medical Sciences, Seton Hall University, South Orange, New Jersey
5
Department of Psychological Sciences, Kent State University, Kent, Ohio
The amount of information that medical students learn is voluminous and those
who do not use evidence-based learning strategies may struggle. Research from
cognitive and educational psychology provides a blueprint on how best to learn sci-
ence subjects, including clinical anatomy. Students should aim for high-cognitive
learning levels as defined in the SOLO taxonomy. Using a real-world example from
a modern clinical anatomy textbook, we describe how to learn information using
strategies that have been experimentally validated as effective. Students should
avoid highlighting and rereading text because they do not result in robust learning
as defined in the SOLO taxonomy. We recommend that students use (1) practice
testing, (2) distributed practice, and (3) successive relearning. Practice testing
refers to nonsummative assessments that contain questions used to facilitate
retrieval (e.g., flashcards and practice questions). Practice questions can be fill-in,
short-answer, and multiple-choice types, and students should receive explanatory
feedback. Distributed practice, the technique of distributing learning of the same
content within a single study session or across sessions, has been found to facili-
tate long-term retention. Finally, successive relearning combines both practice
testing and distributed practice. For this strategy, students use practice questions
to continue learning until they can answer all of the practice questions correctly.
Students who continuously use practice testing, distributed practice, and succes-
sive relearning will become more efficient and effective learners. Our hope is that
the real-world clinical anatomy example presented in this article makes it easier
for students to implement these evidence-based strategies and ultimately improve
their learning. Clin. Anat. 32:156–163, 2019. © 2018 The Authors. Clinical Anatomy published by
Wiley Periodicals, Inc. on behalf of American Association of Clinical Anatomists.
Key words: learning strategies; cognitive psychology; educational psychology;
highlighting; rereading; practice testing; distributed practice;
successive relearning; clinical anatomy; SOLO taxonomy
*Correspondence to: Dr. Anthony V. D’Antoni, Division of Anatomy, Department of Radiology, Weill Cornell Medicine, 1300 York Ave-
nue, Box 47, Room A-520, New York, NY 10065. E-mail:
Received 2 October 2018; Accepted 6 October 2018
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/ca.23298
© 2018 The Authors. Clinical Anatomy published by Wiley Periodicals, Inc. on behalf of American
Association of Clinical Anatomists.
This is an open access article under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs
License, which permits use and distribution in any medium, provided the original work is properly cited, the use
is non-commercial and no modifications or adaptations are made.
, Evidence-Based Approach to Learning Clinical Anatomy 157
“The active recall of a fact from within is, as a seek to promote the relational and extended abstract
rule, better than its impression from without.” levels of learning, as discussed in the SOLO Taxon-
—Thorndike (1906). omy, as deep learning experiences.
The SOLO taxonomy of learning proposed by Biggs
and Collis (1982) is a mechanism to motivate stu-
dents’ development intrinsically and extrinsically, to
INTRODUCTION think reflectively and drive their self-determination to
learn. SOLO taxonomy is a process used to describe
Since the time of Sir William Osler, there have been increasing levels of complexity in a learner’s under-
several opinions on how medical students learn best standing of a concept (Biggs and Collis, 1982). SOLO
and how their learning environments can be improved taxonomy is a five-leveled approach that classifies
(Armstrong et al., 2004; Becker, 2014). Although a few the observed learning outcome as either prestruc-
papers have been published on undergraduate college tural, unistructural, multistructural, relational, or
student learning of anatomy and physiology (Dobson extended abstract (Pinto Zipp et al., 2016). As a
and Linderholm, 2015), none, to our knowledge, have learner moves along these levels, their cognitive abili-
specifically focused on how to use evidence-based ties transition from that of recalling bits of information
strategies to learn clinical anatomy in medical school. to evaluating and synthesizing information, ultimately
This void could be due to the misperception that medi- supporting the transfer of knowledge acquired to new
cal students already use effective strategies because situations. This process of transforming knowledge
they are high-performing students. Although students demonstrates a deeper level of learning (Biggs and
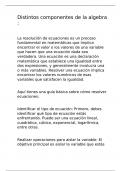
matriculating at U.S. medical schools have high grade Collis, 1982). Figure 1 shows the different levels of
point averages and Medical College Admission Test the SOLO taxonomy (Pinto Zipp et al., 2016). In level
(MCAT) scores (Mitchell, 1990), some struggle in the one, prestructural, the learner acquires unconnected
medical school curriculum. Another obstacle could be a pieces of information and is unsure about the subject
lack of awareness among medical students, educators, matter in general. In level two, unistructural, the
and administrators about research from the field of learner possesses an idea about the information and
cognitive psychology (Ruiter et al., 2012), which has begins to make simple connections between informa-
systematically explored many techniques that promise tion and ideas but no significant associations are
to improve student achievement. formed. In level three, mulitstructural, the learner
The content presented in U.S. medical schools has begins to make several connections among individual
increased exponentially during the last 50 years, even ideas and information, but a meta-connection among
though the duration of the 4 year undergraduate all the information is lacking. In level four, relational,
medical curriculum has remained unchanged the learner begins to see the connections between
(Anderson and Graham, 1980; D’Antoni et al., 2010). the individual parts of the information acquired and
Therefore, there has been increased pressure on how they fit into the whole understanding of the con-
medical students to absorb vast amounts of informa- cept. Finally, in level five, extended abstract, the
tion with limited time. This could be one of the main learner is able to transfer and generalize information
factors influencing their academic success in medical and ideas from one context to another (Biggs and Col-
school coursework. We have observed that the learn- lis, 1982).
ing strategies used by some medical students, espe- Researchers suggest that by using the SOLO tax-
cially during the first year, are not robust enough to onomy, curricula can be aligned to assessments and
meet the challenges associated with deep learning
but rather support surface knowledge acquisition
(D’Antoni et al., 2009). As described in the structure
of observed learning outcomes (SOLO) taxonomy,
deep learning is achieved when the learner moves
from unistructural and multistructural levels (both are
associated with a surface approach to learning) to
rational and extended abstract levels (Hattie and
Brown, 2004). The learning strategies used by the
learner, in this case the medical student, will influence
the level and depth of learning. And depending on the
learner’s goals (retention of critical facts or under-
standing core concepts), different techniques are
likely to be more effective in achieving them.
On the basis of what is currently known regarding
medical school curricula, medical students’ character-
istics, learning theory, learning strategies, and the
adult learner, how can we as educators use learning
strategies that will move medical students from using Fig. 1. Different levels of the SOLO taxonomy and
surface learning experiences to embracing deeper characteristics associated with the learner’s cognitive
learning experiences? We argue in this paper that it is abilities at each level. [Color figure can be viewed at
through modeling the use of learning strategies that wileyonlinelibrary.com]
MEDICAL AND DENTAL EDUCATION
An Evidence-Based Approach to Learning
Clinical Anatomy: A Guide for Medical Students,
Educators, and Administrators
ANTHONY V. D’ANTONI ,1* ESTOMIH P. MTUI,1 MARIOS LOUKAS ,2
R. SHANE TUBBS ,3 GENEVIEVE PINTO ZIPP,4 AND JOHN DUNLOSKY5
1
Division of Anatomy, Department of Radiology, Weill Cornell Medicine, New York, New York
2
Department of Anatomical Sciences, St. George’s University School of Medicine, Grenada, West Indies
3
Seattle Science Foundation, Seattle, Washington
4
Department of Interprofessional Health Sciences and Health Administration, School of Health and
Medical Sciences, Seton Hall University, South Orange, New Jersey
5
Department of Psychological Sciences, Kent State University, Kent, Ohio
The amount of information that medical students learn is voluminous and those
who do not use evidence-based learning strategies may struggle. Research from
cognitive and educational psychology provides a blueprint on how best to learn sci-
ence subjects, including clinical anatomy. Students should aim for high-cognitive
learning levels as defined in the SOLO taxonomy. Using a real-world example from
a modern clinical anatomy textbook, we describe how to learn information using
strategies that have been experimentally validated as effective. Students should
avoid highlighting and rereading text because they do not result in robust learning
as defined in the SOLO taxonomy. We recommend that students use (1) practice
testing, (2) distributed practice, and (3) successive relearning. Practice testing
refers to nonsummative assessments that contain questions used to facilitate
retrieval (e.g., flashcards and practice questions). Practice questions can be fill-in,
short-answer, and multiple-choice types, and students should receive explanatory
feedback. Distributed practice, the technique of distributing learning of the same
content within a single study session or across sessions, has been found to facili-
tate long-term retention. Finally, successive relearning combines both practice
testing and distributed practice. For this strategy, students use practice questions
to continue learning until they can answer all of the practice questions correctly.
Students who continuously use practice testing, distributed practice, and succes-
sive relearning will become more efficient and effective learners. Our hope is that
the real-world clinical anatomy example presented in this article makes it easier
for students to implement these evidence-based strategies and ultimately improve
their learning. Clin. Anat. 32:156–163, 2019. © 2018 The Authors. Clinical Anatomy published by
Wiley Periodicals, Inc. on behalf of American Association of Clinical Anatomists.
Key words: learning strategies; cognitive psychology; educational psychology;
highlighting; rereading; practice testing; distributed practice;
successive relearning; clinical anatomy; SOLO taxonomy
*Correspondence to: Dr. Anthony V. D’Antoni, Division of Anatomy, Department of Radiology, Weill Cornell Medicine, 1300 York Ave-
nue, Box 47, Room A-520, New York, NY 10065. E-mail:
Received 2 October 2018; Accepted 6 October 2018
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/ca.23298
© 2018 The Authors. Clinical Anatomy published by Wiley Periodicals, Inc. on behalf of American
Association of Clinical Anatomists.
This is an open access article under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs
License, which permits use and distribution in any medium, provided the original work is properly cited, the use
is non-commercial and no modifications or adaptations are made.
, Evidence-Based Approach to Learning Clinical Anatomy 157
“The active recall of a fact from within is, as a seek to promote the relational and extended abstract
rule, better than its impression from without.” levels of learning, as discussed in the SOLO Taxon-
—Thorndike (1906). omy, as deep learning experiences.
The SOLO taxonomy of learning proposed by Biggs
and Collis (1982) is a mechanism to motivate stu-
dents’ development intrinsically and extrinsically, to
INTRODUCTION think reflectively and drive their self-determination to
learn. SOLO taxonomy is a process used to describe
Since the time of Sir William Osler, there have been increasing levels of complexity in a learner’s under-
several opinions on how medical students learn best standing of a concept (Biggs and Collis, 1982). SOLO
and how their learning environments can be improved taxonomy is a five-leveled approach that classifies
(Armstrong et al., 2004; Becker, 2014). Although a few the observed learning outcome as either prestruc-
papers have been published on undergraduate college tural, unistructural, multistructural, relational, or
student learning of anatomy and physiology (Dobson extended abstract (Pinto Zipp et al., 2016). As a
and Linderholm, 2015), none, to our knowledge, have learner moves along these levels, their cognitive abili-
specifically focused on how to use evidence-based ties transition from that of recalling bits of information
strategies to learn clinical anatomy in medical school. to evaluating and synthesizing information, ultimately
This void could be due to the misperception that medi- supporting the transfer of knowledge acquired to new
cal students already use effective strategies because situations. This process of transforming knowledge
they are high-performing students. Although students demonstrates a deeper level of learning (Biggs and
matriculating at U.S. medical schools have high grade Collis, 1982). Figure 1 shows the different levels of
point averages and Medical College Admission Test the SOLO taxonomy (Pinto Zipp et al., 2016). In level
(MCAT) scores (Mitchell, 1990), some struggle in the one, prestructural, the learner acquires unconnected
medical school curriculum. Another obstacle could be a pieces of information and is unsure about the subject
lack of awareness among medical students, educators, matter in general. In level two, unistructural, the
and administrators about research from the field of learner possesses an idea about the information and
cognitive psychology (Ruiter et al., 2012), which has begins to make simple connections between informa-
systematically explored many techniques that promise tion and ideas but no significant associations are
to improve student achievement. formed. In level three, mulitstructural, the learner
The content presented in U.S. medical schools has begins to make several connections among individual
increased exponentially during the last 50 years, even ideas and information, but a meta-connection among
though the duration of the 4 year undergraduate all the information is lacking. In level four, relational,
medical curriculum has remained unchanged the learner begins to see the connections between
(Anderson and Graham, 1980; D’Antoni et al., 2010). the individual parts of the information acquired and
Therefore, there has been increased pressure on how they fit into the whole understanding of the con-
medical students to absorb vast amounts of informa- cept. Finally, in level five, extended abstract, the
tion with limited time. This could be one of the main learner is able to transfer and generalize information
factors influencing their academic success in medical and ideas from one context to another (Biggs and Col-
school coursework. We have observed that the learn- lis, 1982).
ing strategies used by some medical students, espe- Researchers suggest that by using the SOLO tax-
cially during the first year, are not robust enough to onomy, curricula can be aligned to assessments and
meet the challenges associated with deep learning
but rather support surface knowledge acquisition
(D’Antoni et al., 2009). As described in the structure
of observed learning outcomes (SOLO) taxonomy,
deep learning is achieved when the learner moves
from unistructural and multistructural levels (both are
associated with a surface approach to learning) to
rational and extended abstract levels (Hattie and
Brown, 2004). The learning strategies used by the
learner, in this case the medical student, will influence
the level and depth of learning. And depending on the
learner’s goals (retention of critical facts or under-
standing core concepts), different techniques are
likely to be more effective in achieving them.
On the basis of what is currently known regarding
medical school curricula, medical students’ character-
istics, learning theory, learning strategies, and the
adult learner, how can we as educators use learning
strategies that will move medical students from using Fig. 1. Different levels of the SOLO taxonomy and
surface learning experiences to embracing deeper characteristics associated with the learner’s cognitive
learning experiences? We argue in this paper that it is abilities at each level. [Color figure can be viewed at
through modeling the use of learning strategies that wileyonlinelibrary.com]